Download as PDF, PPTX



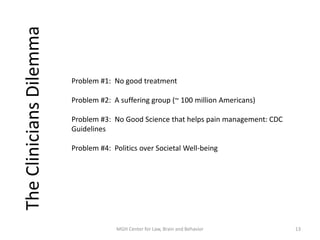

The document discusses the challenges in managing chronic pain with opioids, highlighting the lack of effective treatments and the significant impact of opioid addiction on both patients and society. It cites the economic burden of chronic pain, the prevalence of mental health issues among those affected, and the insufficient evidence regarding the safety and efficacy of long-term opioid therapy. The text also emphasizes the need for better research, data, and public policy to address these complex issues.