High Profile Call Girls Jaipur Vani 8445551418 Independent Escort Service Jaipur
gout.pptx
1. 1
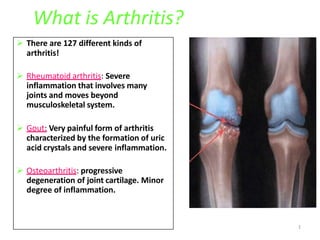
What is Arthritis?
There are 127 different kinds of
arthritis!
Rheumatoid arthritis: Severe
inflammation that involves many
joints and moves beyond
musculoskeletal system.
Gout: Very painful form of arthritis
characterized by the formation of uric
acid crystals and severe inflammation.
Osteoarthritis: progressive
degeneration of joint cartilage. Minor
degree of inflammation.
3. metabolic disorder
• Gout is a
metabolism,
of purine
characterized by intermittent
attacks of acute pain, swelling and
inflammation.
• It always preceded by hyperuricaemia (6.0mg/dl)
Hyperuricaemia due to excessive amount of uric
acid production or decreased excretion
4. • Hyperuricaemia - primary or secondary.
• Primary hyperuricaemia classified as
“Overproducers” or “under execrators”
5. • Primary Hyperuricemia and
Gout with No Associated
Condition
• Uric acid undersecretion(80%–
90%)
• Idiopathic
• Urate overproduction (10%–
20%)
• HGPRT deficiency
• PRPP synthetase overactivity
• (Phasphoribosyl pyrophosphate)
Secondary Hyperuricemia and Gout with
Identifiable Associated Condition
• develop during course of other diseases
(Leukaemias, lymphomas, chemotherapy)
• Some drug therapy (Thiazide diuretics,
furosamide, ethacrynic acid)
• Some disorders Diabeticketoacidosis, lead
poison, Lymphoproliferative
diseases, Hemolytic anemias, psoriasis
• Dual mechanism
Obesity, Hypoxemia and hypoperfusion
6. Uric acid production and excretion
RNA,DNA
PURINES
HYPOXANTHINES
XANTHINES
URIC ACID (low water soluble)
Uric acid freely filtrated through by glomerulus and
reabsorbed by tubular fluid
Xanthine oxidase
Xanthine oxidase
Probencid
PRPP
Hyperuricemia Gout Deposits of urate crystal Nephrolithiasis
7. Pathophysiology of gout
Uricacid
Blood
React with sodium
Sodium crystals (tophi)
Deposited in soft tissues and joints
Inflammation(ry)
Infiltration of granulocytes that phagocytise the urate crystals
Generate free radicals
Free radical damage the tissue
Release of proteolytic enzyme glycoprotein
Release of lactic acid
More ppt of urate crystals
Indomethacin
Colchicine
Colchicine
Colchicine
Release of lysosomal enzymes
Destruction of joints
8. Acute gout
• Painful arthritic attack of sudden onset.
• Usually occurring at night or in early morning
• Arthritic pain worsen progressively
• Generally involves one or few joints
• Most common site of initial attack metatarsophalangeal
joint.
• Other sites ankle, heel, knee, wrist, elbow and fingers.
9. Chronic gout
• Frequency of attacks increases, continuous deposit leads
to damage joints and chronic pain
• Patients may develop large subacutenous tophi (Stones)
in pinna of external ear, eyelids, nose and around joints
• The ureate crystals in kidney leads renal disease.
• Articular cartilage may be destroyed result in joint
deformities
12. Colchicine
• Alkaloid from colchium autumnale. (1973)
• Neither analgesic nor anti inflammatory, but specific
for gouty inflammation.
• It is only effective in prophylaxis of acute gout
• It has no effect on synthesis or promote excretion
• MOA
• Colchicine binds to intracellular protein ‘Tubulin’ and
causes depolymerisation and disappearance of
microtubules in granulocytes & Inhibit granulocyte
migration so decrease phagocytic activity
13. • Colchicine inhibit glycoprotein release
– Other actions-
- arrest of mitosis in metaphas “spindle poison”
- increases gut motility.
- Antipyretic , respiratory depressant
- Inhibit histamine , Insulin release
- hypertensive at high dose , Increase vasomotor tone
- direct vasoconstrictor
14. Uses
Colchicine preferred in pts without confirmed diagnosis of
gout.
Acute gout-1mg orally followed by 0.25 mg 3 hrly till control.
(EHC) 3-7days
With safer alternatives NSAIDs use of Colchicine have declined
ADR:- diarrhoea, vomiting, abdominal pain.
Acute toxicity - bloody diarrhoea, throat pain, respiratory
depression, haematuria.
Chornic toxicity- agranulocytosis, peripheral neuritis and
myopathy, renal tubular necrosis.
15. NSAIDs
• Strong anti inflammatory drugs
• Use in patients without contraindication
• Use maximum dose/potent NSAID
e.g., Indomethacin 50 mg po t.i.d.
Diclofenac 50 mg po t.i.d.
Ketorolac 10 mg q4-6hrsr,
Napoxen, Piroxicam
• continue until pain/inflammation absent for 48 hours
• MOA: inhibit urate crystal phagocytosis and chemotatic
migration of leukocytes into inflammed joints.
• NSAIDs are not recommended for long term.
• (Salicylates are not used , have tendency to raise uric acid)
16. Corticosteroid
Use when NSAIDS/Cholchicine risky or contraindicated
e.g.,: elderly
hypertensive
peptic ulcer disease
renal impairment
liver impairment
use when • NSAIDS ineffective
Mode of administration –
• intra articular - Depomedrol 40-80 mg with lidocaine.
• Oral Prednisone 30-40 mg qd for 3-4 days, taper by 5 mg
every 2-3 days & stop over 1-2 wks
18. • Allopurinol prevents the synthesis of uric acid
by inhibiting the enzyme Xanthine oxidase,
result reduce plasma ureate levels.
• Inc. xanthine ,hypoxanthines are excreted
through urine
• Allopurinol short acting competitive inhibitor
• Metabolite alloxanthine is long acting t1/2 24hr.
19. • Start low 50-100 mg qd
• Increase by 50-100mg every 2-3 weeks according to
symptoms
– “Average” dose 300 mg daily
– lower dose if renal/hepatic insufficiency
– higher dose in non-responders
– prophylactic colchicine until allopurinol dose stable
• Indications:
• Chronic gout
• In patients 24 hrs urinary acid excretion exceeds 1.1g
• For recurrent renal ureate stones.
21. Allopurinol drug interactions
• Allopurinol prolong ½ life of Vidarabine, Cyclosporin
drugs and increase toxicity
• Dec. metabolism of 6-mercaptopurine, Azothiaprine
inc. its effects.
• Interferes with the mobilization of hepatic iron stores -
heamtonic should be avoided during allopurinol
therapy.
22. Uricosuric drugs: (probencid)
•Highly lipid soluble benzoic acid.
•It blocks reabsorption of urate in proximal tubule by
blocking transport (Bidirectional transport)
•PK: Dose dependent t1/2 life
•Dose -250- 500mg b.d. with plenty of fluids, alkalinization
of urine.
Uses :
chronic gout along with NSAIDs / colchicine for
initial 1-2 months.
23. Sulfinpyrazone
• It is a Pyrazolone derivaties related to
Phenylbutazone.
• Inhibits tubular reabsorption of uric acid at
therapeutic doses.
• Its action is additive with probenecid.
• Use -chronic gout
• Dose :100-200mg BD gradually increase
according to the response.
24. • It is newer and more potent uricosuric drug
• Used in patients allergic to probenecid or sulfinpyrazone
• It is reversible inhibitor of tubler reabsorption
• Effective dose 60-80mg/day
• With allopurinol more effective
Benzbromarone