2. HISTAMINES
• Introduction- Autacoids
• Histamine sites
• Synthesis storage and destruction
• Release of Histamine
• Histamine Receptors and types
• Pharmacological action with sites
• Pathophysiological roles of Histamines
• Uses of Histamine
3. ANTIHISTAMINES
• Histamine Antagonists
• Classification H1 Antagonists
• Second generation Antihistamines
• Pharmacological effects
• Mechanism of action
• Pharmacokinetics
• Therapeutic uses and Side effects
• Drug interactions
• H2 Antagonist & Pharmacological effects
• Drugs , Mechanism of action, Uses
4. INTRODUCTION-
AUTACOIDS
• AUTACOIDS auto=self akos=healing/remedy
• First autacoid to be discovered
• Histamine was synthesized in 1907 and
characterized in 1910
• Demonstrated to be a natural constituent of
mammalian tissues(1927)
• These are diverse substances produced by a
wide variety of cells in the body, having intense
biological activity, but generally act locally (e.g.
within inflammatory pockets) at the site of
synthesis and release.
• Thus they have also been called ‘local
hormones’
5. AUTACOIDS
• Autacoids are involved in a number
of physiological and pathological
processes (especially reaction to injury
and immunological insult)
• And even serve as transmitters or
modulators in the nervous system, but
their role at many sites is not precisely
known.
• A number of useful drugs act by
modifying their action or metabolism.
6. CLASSIFICATION
Amine derived: Histamine (amino acid:
Histidine), Serotonin (5 hydroxy tryptamine)
Peptide derived: Plasmakinins (Bradykinin,
Kallidin), Angiotensin
Lipid derived: Prostaglandins, Leukotrienes,
Platelet Activating Factor (PAF), etc.
Others : Cytokines (interleukins, TNFα, GM-
CSF, etc.) and several peptides like gastrin,
somatostatin, vasoactive intestinal peptide
(VIP) and many others may be considered as
autacoids.
7. HISTAMINES
• Histamine, meaning ‘tissue amine’ (histos—tissue)
• Imidazole ethylamine -formed from the amino acid Histidine
• Important inflammatory mediator
• Plays an important role in inflammation, anaphylaxis, allergies, gastric acid
secretion, neurotransmission in parts of the brain and drug reaction
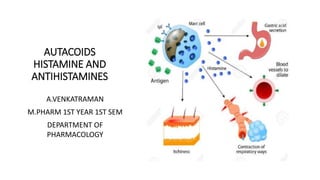
• As part of an immune response to foreign pathogens, its produced by
Basophils and Mast cells found in nearby connective tissues.
8. SITES OF
HISTAMINE
Mast cell site:
• Pulmonary tissue (mucosa of bronchial tree)
• Skin
• GIT(intestinal mucosa), lung, liver and placenta
Concentration of histamine is particularly high in
these tissues
Non-mast cell sites:
• CNS (neurons)
• Epidermis of skin.
• GIT(gastric cells)
• Cells in regenerating or rapidly growing tissues
• Basophils (in the blood)
10. STORAGE AND DEGRADATION
Stored in complex with:
• Heparin
• Chondroitin sulphate
• Eosinophilic Chemotactic Factor
• Neutrophilic Chemotactic Factor
Proteases Degradation:
• Degraded rapidly by oxidation to imidazole acetic acid
• Degraded rapidly by methylation to N-methyl histamine
• Very little histamine is excreted unchanged
11.
12. RELEASE OF
HISTAMINES:
1. Tissue injury:
Any physical or chemical agent that injures tissue, skin
or mucosa are particularly sensitive to injury and will
cause the immediate release of histamine from mast
cells.
• Chemical and mechanical mast cell injury causes
degranulation and histamine release
• Surface acting agents like Tween 80, compound 48/
80 etc. The primary action of these substances is
release of histamine from mast cells, therefore they
are called histamine liberators.
• They produce an ‘anaphylactoid’ reaction—itching
and burning sensation, flushing, urticaria, fall in BP,
tachycardia, headache, colic and asthma.
13. 2. Allergic reactions:
• Exposure of an antigen to a
previously sensitized (exposed)
subject can immediately trigger
allergic reactions.
• If sensitized by IgE antibodies
attached to their surface
membranes will degranulate when
exposed to the appropriate
antigen and release histamine, ATP
and other mediators
14. 3. Drugs and other foreign
compounds:
Morphine, dextran,
antimalarial drugs, dyes,
antibiotic bases, alkaloids,
amides, quaternary
ammonium compounds,
enzymes (phospholipase C).
Penicillins, Tetracyclines, Basic
drugs- amides, amidines,
diamidines, Toxins, venoms,
Proteolytic enzymes,
Bradykinin, Kallidin, and
Substance P
16. HISTAMINE RECEPTORS- Subtypes
Histaminergic receptors were classified by Asch and Schild (1966) into H1 & H2
H1 receptors: Mediate effects on smooth muscle leading to vasodilation (relaxation of
vascular smooth muscle), increased permeability and contraction of non-vascular smooth
muscle
Sir James Black (1972) developed the first H2 blocker burimamide
H2 receptors: Mediate histamine stimulation of gastric acid secretion and may be involved
in cardiac stimulation
H3 receptor, which serves primarily as an autoreceptor controlling histamine release from
neurons in brain was identified in 1983.
H3 receptor : Feedback inhibition in CNS, GIT, Lungs and Heart
Molecular cloning has revealed yet another (H4 ) receptor in 2001
H4 receptors: Eosinophils, Neutrophils and CD4 T-cells
All these four receptors are members of the 7-transmembrane (heptahelical) spanning
family of receptors, are G protein-coupled (GPCR)
17.
18.
19. PHARMACOLOGICAL
ACTIONS-H1
BLOOD VESSELS:
•C5a and C3a stimulate mast cells to release Histamine,
that causes marked dilatation of smaller blood vessels,
including arterioles, capillaries and venules.
• Like ACh and many other autacoids, vasodilatation
caused by histamine is partly (H1 component) indirect,
mediated through ‘endothelium dependent relaxing factor’
(EDRF)
• If Injected intradermally, it elicits the triple response
consisting of:
Red spot: due to intense capillary dilatation.
Wheal: due to exudation of fluid from capillaries and
venules.
Flare: redness in the surrounding area due to arteriolar
dilatation mediated by axon reflex.
20. Exocrine Excretion(H1):
•Increased production of nasal and bronchial mucus
Bronchial Smooth Muscle(H1)
•Bronchiolar constriction
•Asthmatic symptoms
•Decreased Lung capacity
Intestinal Smooth Muscle(H1)
• Contraction - Intestinal cramps and diarrhea
Sensory Nerve Endings(H1)
• Itching and pain
Central Nervous System
• Histamine does not penetrate blood brain barrier—no central effects are seen on I V injection.
However, intra cerebro ventricular administration produces rise in BP, cardiac stimulation,
behavioral arousal, hypothermia, vomiting and ADH release. These effects are mediated through
both H1 and H2 receptors
21. Pharmacological
Actions (H1&H2):
Cardiovascular System (H1&H2)
• Decreased Peripheral resistance -----
decreased systemic BP
• Positive chronotropism(H2)
• Positive inotropism
Skin (H1&H2)
• Dilatation and increased permeability of the
venules
• Leakage of fluid + proteins into the tissues
• Classic “triple-response”
22. Histamine- Pathophysiological roles:
GASTRIC SECRETION:
• Histamine has dominant physiological
role in mediating secretion of Hcl in
stomach.
• It is released locally under the influence
of all stimuli that evoke gastric secretion
(feeding, vagal stimulation, cholinergic
drugs and gastrin) and activates the
proton pump (H+K+ ATPase) through H2
receptors.
• H2 blockers not only suppress acid
secretion induced by histamine but also
markedly diminish that in response to
ACh and gastrin.
23. Allergic Phenomena:
Released from mast cells following AG : AB reaction on their surface (involving IgE type
of reaginic antibodies;) in immediate type of hypersensitivity reactions, histamine is
causative in urticaria, angioedema, bronchoconstriction and anaphylactic shock.
As Transmitter:
Histamine is believed to be the afferent transmitter which initiates the sensation of itch
and pain at sensory nerve endings.
• In the brain H1 agonist suppresses appetite; certain H1 antagonists stimulate
appetite.
• Histamine also appears to act as a transmitter regulating body temperature,
cardiovascular function, thirst, hormone release from anterior pituitary and possibly
other functions
24. Inflammation:
• Histamine has been implicated as a mediator of vasodilatation and other changes
that occur during inflammation.
• It promotes adhesion of leukocytes to vascular endothelium by expressing
adhesion molecule P-selectin on endothelial cell surface, sequestrating leukocytes
at the inflammatory site.
Tissue Growth and Repair:
Because growing and regenerating tissues contain high concentrations of histamine, it
has been suggested to play an essential role in the process of growth and repair.
Headache:
Histamine has been implicated in certain vascular headaches, but there is no
conclusive evidence.
25. USES-
HISTAMINE
• No therapeutic value
• Occasionally used in some diagnostic tests:
• Testing gastric acid secretion.
• Diagnosis of Phechromocytoma.
• Pulmonary function: to test for bronchial
hyperreactivity.
Betahistine - H1 agonist
• Used to control vertigo in patients of meniere’s disease.
• Acts by causing Vasodilatation in internal ear.
• It is contraindicated in asthmatics and ulcer patients.
Betazole - H2 agonist
• Used in gastric function tests
28. H1 ANTIHISTAMINES
The term antihistamine, refers to the classic H1- receptor blockers
These compounds do not influence the formation or release of histamine;
rather, they block the receptor mediated response of a target tissue
These drugs competitively antagonize actions of histamine at the H1
receptors
30. H1 ANTIHISTAMINES - GENERATIONS
• The H1-receptor blockers can be divided into : First and Second
generation drugs.
• The first generation drugs penetrate the CNS and cause sedation
• The second generation agents are specific for H1 receptors
• Because they do not penetrate the blood-brain barrier, they show less
CNS toxicity than the first-generation drugs
• Among these agents loratadine/ desloratadine/ fexofenadine produce
the least sedation
31.
32. H1 Antihistamines- Second generation drugs
Fexofenadine:
• It is the active metabolite of terfenadine
• Fexofenadine does not cross blood-brain barrier—does not produce
sedation or impair psychomotor performance
• It is rapidly absorbed, excreted unchanged in urine and bile, has
plasma t½ 11– 16 hours and duration of action 24 hours
• Dose: For allergic rhinitis 120 mg OD; for urticaria and other skin
allergies 180 mg OD.
33. Loratadine
• Selective peripheral H1 antagonist which lacks CNS depressant effects
and is fast acting.
• No interaction with macrolides or antifungals has been noted. Good
efficacy has been reported in urticaria and atopic dermatitis.
Desloratadine
• It is the major active metabolite of loratadine effective at half the
dose
• Noninterference with psychomotor performance and cardiac safety
are documented.
34. PHARMACOLOGICAL EFFECTS OF
ANTIHISTAMINES
Sedation
• A common effect of first-generation H1 antagonists is sedation, but
the intensity of this effect varies among chemical subgroups.
• Second-generation H1 antagonists have little or no sedative or
stimulant actions
COUGH
• Antihistaminics like chlorpheniramine, diphenhydramine and
promethazine are constituents of many popular cough remedies
35. PHARMACOLOGICAL EFFECTS
OF ANTIHISTAMINES
Acute muscle dystonia Caused by antidopaminergic-antipsychotic drugs is
promptly relieved by parenteral promethazine, diphenhydramine or
hydroxyzine.
Antihistaminics block symptoms produced by histamine liberators; afford
symptomatic relief in insect bite and ivy poisoning
Antinausea and Antiemetic Actions
• Several first- generation H1 antagonists have significant activity in
preventing motion sickness.
• They are less effective against an episode of motion sickness already
present
ALSO HAS ANTIPARKINSON EFFECTS
36. PHARMACOKINECTICS
Absorption
These agents are rapidly absorbed after oral administration
• Peak blood concentrations occur in 1–2 hours
• Widely distributed throughout the body
• First-generation drugs enter CNS readily
Biotransformation(Metabolism)
Some of them are extensively metabolized, primarily by microsomal
systems in the liver
• Several of the second-generation agents are metabolized by the
CYP3A4 system
37. Antihistamines-
Therapeutic
Uses and
• Used in the treatment of allergy and
inflammatory conditions
MOTION SICKNESS
Diphenhydramine, dimenhydrinate,
cyclizine, meclizine, and hydroxyzine,
are the most effective agents for
prevention of the symptoms of motion
sickness
• USED IN THE TREATMENT OF
VERTIGO
39. DRUG INTERACTIONS
Antihistamines that produce
sedation can potentiate CNS
depressants (e.g., barbiturates,
opiates, general anesthetics,
and alcohol)
Antihistamines that possess
anticholinergic actions can
produce manifestations of
excessive blockade if given with
anticholinergic drugs (e.g., dry
mouth, constipation, or blurred
vision)
40. H2
ANTAGONIST
The first H2 blocker
Burimamide was
developed by Black
in 1972.
Metiamide was the
next.
Cimetidine was
introduced in 1977
and gained wide
usage.
Ranitidine,
famotidine,
roxatidine, and
many others have
been added
subsequently.
They are primarily
used in peptic
ulcer and other
gastric
hypersecretory
states
41. Regulation of Gastric acid secreation
H2 antagonists suppress not
only histamine, but also ACh,
gastrin and in fact any gastric
acid secretory stimulus.
42. H2 Antagonist Pharmacological Effects
Cimetidine and all other H2 antagonists block histamine-induced gastric secretion,
cardiac stimulation
• They attenuate fall in BP due to histamine, especially the late phase response
seen with high doses.
• They are highly selective: have no effect on H1 mediated responses or on the
action of other transmitters/autacoids.
• The H2 blockers have antiulcerogenic effect. Gastric ulceration due to stress and
drugs (NSAIDs, cholinergic, histaminergic) is prevented.
• Reduces gastric acid volume and concentration of pepsin
43. Ranitidine
• A nonimidazole (has a furan ring) H2 blocker, it has several desirable
features compared to cimetidine:
• About 5 times more potent than cimetidine.
H2 Antagonist- Therapeutic Uses
• Duodenal ulcer
• Gastric ulcer
• Zollinger-Ellison syndrome (a pathological hypersecretory state
resulting in excessive gastric pepsin & HCl)
• Gastroesophageal reflux disease (GERD)