General Preoperative &Postoperative Care of Surgical Patients
TheDay
1. Published November 01. 2010 2:03AM | Updated November 01. 2010 10:10AM
L&M enters new era with first
gastric bypass surgery
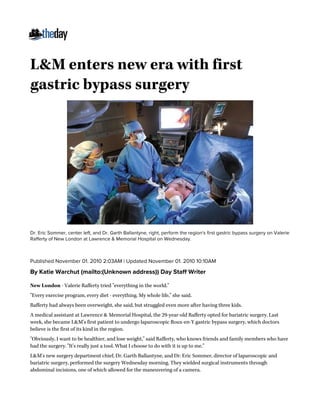
Dr. Eric Sommer, center left, and Dr. Garth Ballantyne, right, perform the region's first gastric bypass surgery on Valerie
Rafferty of New London at Lawrence & Memorial Hospital on Wednesday.
By Katie Warchut (mailto:(Unknown address)) Day Staff Writer
New London - Valerie Rafferty tried "everything in the world."
"Every exercise program, every diet - everything. My whole life," she said.
Rafferty had always been overweight, she said, but struggled even more after having three kids.
A medical assistant at Lawrence & Memorial Hospital, the 29-year-old Rafferty opted for bariatric surgery. Last
week, she became L&M's first patient to undergo laparoscopic Roux-en-Y gastric bypass surgery, which doctors
believe is the first of its kind in the region.
"Obviously, I want to be healthier, and lose weight," said Rafferty, who knows friends and family members who have
had the surgery. "It's really just a tool. What I choose to do with it is up to me."
L&M's new surgery department chief, Dr. Garth Ballantyne, and Dr. Eric Sommer, director of laparoscopic and
bariatric surgery, performed the surgery Wednesday morning. They wielded surgical instruments through
abdominal incisions, one of which allowed for the maneuvering of a camera.
2. Watching their work on video screens, they stapled off a small portion of the stomach to make a pouch. They
connected the smaller part of the stomach to the middle of the small intestine so that food will bypass the rest of
the stomach and top of the small intestine.
The procedure is restrictive because it makes the stomach smaller and is considered a malabsorption procedure,
meaning the person absorbs fewer calories, Sommer said. They have also found it leads to hormonal changes such
as a decrease in ghrelin, a hormone that causes hunger.
The patient consumes only liquids for two weeks and then only soft foods for another two. The person can take in
only 200 to 300 calories per day and gradually increases to 1,000 after a year. Average weight loss is about 75 percent
of excess weight; a person who is 100 pounds overweight would lose about 75. The patient must take vitamins to
make up for deficiencies.
With Rafferty's body mass index of 40, the minimum threshold for the surgery, the doctors expect she can drop
about 70 pounds to a weight of 170.
Rafferty is a prime example of why Ballantyne, who came from Hackensack University Medical Center in New
Jersey, wanted to bring bariatric surgery to L&M. She had been working with a doctor in New Haven but had a hard
time making the trip there and ran into insurance issues.
Ballantyne said 400 people a year were leaving southeastern Connecticut to go to other hospitals for the surgery.
"If we captured all those people, it would be the most commonly performed procedure at the hospital," he said.
It also provides a service for those who have already had the operations but need close follow-up care. Ballantyne
believes the surgery fits in with the definition of a community hospital, which "should provide excellent care for
patients for the epidemics of our time." Obesity is the leading epidemic of the 21st century, he said, as about 40
percent of Americans suffer from the condition, which can lead to other health care issues.
But Rafferty knows it's not a simple fix.
"I just had Chinese food with the girls," she said the day before the surgery, "and I thought, I'll never be able to eat
this again. I'm from an Italian family; we nurture with food. I have to change the way I cook, the recipes, reading
labels when I go grocery shopping."
Ballantyne said if patients eat too much, "they get an immediate response," meaning vomiting. Because there's no
longer room in the stomach for both drinks and solid food, a patient has to wait between drinking and eating.
To that end, patients have to be evaluated to make sure they're not emotionally and psychologically compelled to
eat, he said.
Doctors ask, "What's your relationship with food? You need to understand you're giving up food for this operation.
Are you prepared to do that?" he said.
Ballantyne, whose hospital in Hackensack was the second- busiest bariatric surgery center in the United States,
performing as many as 1,000 operations per year, led L&M through the process to begin offering the surgery in New
London.
The hospital brought in a consultant from the hospital in Hackensack to coordinate issues such as sensitivity
training for staff, since morbidly obese people often face discrimination, and to ensure that the hospital's
equipment can accommodate larger people.
A goal is to obtain designation as a "center of excellence," which will allow the hospital to accept Medicare and
Medicaid patients.
The first procedure took about 2 hours and 15 minutes, about 20 minutes longer than usual, and the staff learned
they'd have to bring in some more equipment, but it was otherwise a success.
"It's sort of like a team sport," Ballantyne said. "They did a great job today."
3. L&M also offers two other types of bariatric surgery - laparoscopic adjustable gastric banding, which places an
adjustable silicone band around the upper part of the stomach, and the fairly new sleeve gastrectomy, which staples
off the stomach into the shape of a banana and removes the unused portion. The type of surgery is the patient's
choice. Gastric bypass is the most common, but banding is catching up, Ballantyne said.
The William W. Backus Hospital in Norwich offers laparoscopic adjustable banding, according to a hospital
spokesman, and has completed three so far, with others scheduled.
FYI
Information sessions are held on the second and fourth Thursday each month at 4 to 6 p.m. at 4
Shaw's Cove, Suite #201, New London.
For more information visit www.lapsurgery.com (http://www.lapsurgery.com).