Aushad detail of dr nagraj
•Download as DOC, PDF•
0 likes•77 views

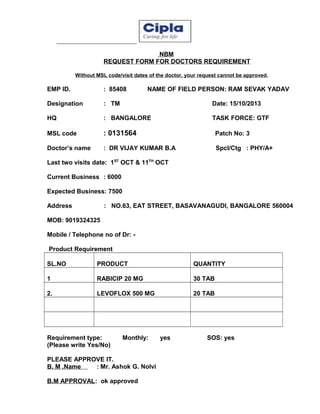
The document is a request form submitted by a field person to their branch manager seeking approval to provide products to a doctor. It includes details of the doctor such as name, specialization, last two visit dates, current and expected business. It lists the requested products and quantities along with whether it is a monthly or SOS requirement. The branch manager approves the request and comments that providing this service can gain better support from the doctor as they are potential for the company's products.

More Related Content
Aushad detail of dr nagraj
- 1. NBM REQUEST FORM FOR DOCTORS REQUIREMENT Without MSL code/visit dates of the doctor, your request cannot be approved. EMP ID. : 85408 NAME OF FIELD PERSON: RAM SEVAK YADAV Designation : TM Date: 15/10/2013 HQ : BANGALORE TASK FORCE: GTF MSL code : 0131564 Patch No: 3 Doctor’s name : DR VIJAY KUMAR B.A Spcl/Ctg : PHY/A+ Last two visits date: 1ST OCT & 11TH OCT Current Business : 6000 Expected Business: 7500 Address : NO.63, EAT STREET, BASAVANAGUDI, BANGALORE 560004 MOB: 9019324325 Mobile / Telephone no of Dr: Product Requirement SL.NO PRODUCT QUANTITY 1 RABICIP 20 MG 30 TAB 2. LEVOFLOX 500 MG 20 TAB Requirement type: (Please write Yes/No) Monthly: PLEASE APPROVE IT. B. M .Name : Mr. Ashok G. Nolvi B.M APPROVAL: ok approved yes SOS: yes
- 2. Comments by BM: - doctor is potential for Spectra care product and after giving this service we can get better support from the doctor.