La Mondialisation de la Santé Mentale / Mental Health Goes Global
•
1 like•642 views

Cet article bilingue (français/anglais) pour le Journal de l'AMPQ - Volume 20, No. 4, Décembre 2017, pp. 21-23 - annonce la Conférence scientifique de l'American Psychiatric Association Filiale québécoise à Montréal le 19 janvier 2018 au sujet de la Santé mentale globale. This bilingual article (English/French) for the Journal of the AMPQ, Volume 20, No. 4, Décembre 2017, pp. 21-23, announces the Annual Scientific Meeting of the Quebec & Eastern Canada District Branch of the American Psychiatric Association in Montreal on January 19th, 2018.

Recommended
Recommended
More Related Content
Similar to La Mondialisation de la Santé Mentale / Mental Health Goes Global
Similar to La Mondialisation de la Santé Mentale / Mental Health Goes Global (20)
More from Université de Montréal
More from Université de Montréal (20)
Recently uploaded
Recently uploaded (11)
La Mondialisation de la Santé Mentale / Mental Health Goes Global
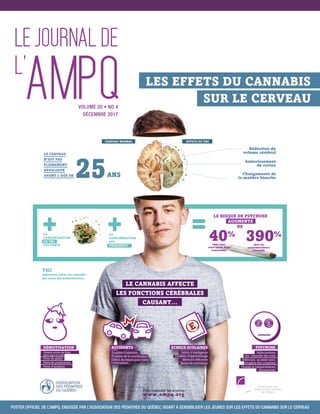
- 1. EFFETS DU THCCERVEAU NORMAL Réduction du volume cérébral Amincissement du cortex Changements de la matière blanche LE CERVEAU N’EST PAS PLEINEMENT DÉVELOPPÉ AVANT L’ÂGE DE 40% chez tous ceux ayant déjà consommé 390% chez les consommateurs intensifs LE RISQUE DE PSYCHOSE AUGMENTE DE ANS25 LA CONCENTRATION EN THC EST FORTE THC Substance active du cannabis qui cause des hallucinations. + + =LA CONSOMMATION EST FRÉQUENTE LE CANNABIS AFFECTE LES FONCTIONS CÉRÉBRALES CAUSANT... ACCIDENTS Troubles d’attention Troubles de la coordination Déficit de vitesse pour traiter l’information PSYCHOSE Hallucinations (ex.: entendre des voix) Délire (ex.: se sentir suivi, imaginer des complots) Pensée et comportements désorganisés ÉCHECS SCOLAIRES Déficit d’intelligence Troubles d’apprentissage Mémoire déficiente Baisse de motivation E Pour consulter les sources: www.ampq.org LES EFFETS DU CANNABIS SUR LE CERVEAU DÉMOTIVATION Jamais envie de faire quoi que ce soit Perte de plaisir Perte de productivité Perte d’ambition VOLUME 20 • NO 4 DÉCEMBRE 2017 POSTER OFFICIEL DE L’AMPQ, ENDOSSÉ PAR L’ASSOCIATION DES PÉDIATRES DU QUÉBEC, VISANT À SENSIBILISER LES JEUNES SUR LES EFFETS DU CANNABIS SUR LE CERVEAU
- 2. VOLUME 20 • NO 4 DÉCEMBRE 2017 ÉDITION Karine J. Igartua, M.D. / ampq@fmsq.org COMITÉ DE RÉDACTION Karine J. Igartua, M.D., Martine Dériger RÉDACTION Amal Abdel-Baki, M.D., Nicolas Bergeron, M.D., Laurent Coulloudon, M.D., Vincenzo Di Nicola, M.D., Ph.D., Simon Dubreucq, M.D., Karine J. Igartua, M.D., Didier Jutras-Aswad, M.D., Sophie L’Heureux, M.D., Richard Montoro, M.D., David Olivier, M.D., Clairélaine Ouellet-Plamondon, M.D.,Aldanie Rho, M.D., Jacynthe Rivest, M.D., Annie Trépanier, M.D., Marie Villeneuve, M.D. COORDINATION DE L’ÉDITION Caroline Piecha CONCEPTION GRAPHIQUE, PRODUCTION ET IMPRESSION Formidée communications TRADUCTION Michel Savage, traducteur ASSOCIATION DES MÉDECINS PSYCHIATRES DU QUÉBEC 2, Complexe Desjardins, Tour de l’Est, 30e étage, Montréal, QC H5B 1G8 Tél. : 514 350-5128 Téléc. : 514 350-5198 ampq@fmsq.org Le Journal est publié par l’Association des médecins psychiatres du Québec (AMPQ). Il paraît 6 fois par année, incluant une édition hors-série «spécial congrès» qui est publiée en début d’année. Le Journal est expédié par courrier à l’ensemble des membres de l’AMPQ. Le contenu de Le Journal ne peut être reproduit, en tout ou en partie, sans l’autorisation de l’éditeur. Les propos tenus dans cette revue et le contenu des publicités n’engagent que leur auteur et en aucun cas l’AMPQ ne pourra être tenue responsable de leur incidence. DÉPÔT LÉGAL 3e TRIMESTRE 2001 Bibliothèque nationale du Canada ISSN 1206-6249. Mot de la présidente 3 Message from the President MOT DU PRÉSIDENT DU COMITÉ DE DÉVELOPPEMENT 7 PROFESSIONNEL MESSAGE FROM THE PRESIDENT OF THE PROFESSIONNAL DEVELOPMENT COMMITTEE CONSULTATION-LIAISON : PETITS TRUCS FONDÉS SUR LES 8 DONNÉES PROBANTES POUR LE PSYCHIATRE GÉNÉRAL QUI COURT TOUJOURS CONSULTATION-LIAISON:TIPS BASED ON CONCLUSIVE DATA FOR THE PSYCHIATRIST ON THE RUN UN DÉBAT FUMANT 11 A FUMING DEBATE FUMER UN PEU, BEAUCOUP,À LA FOLIE OU PAS DU TOUT 13 SMOKE A LITTLE, MORE,A LOT, OR NOT AT ALL LA LÉGALISATION DU CANNABIS : OPPORTUNITÉS ET DÉFIS 17 LEGALIZATION OF CANNABIS: OPPORTUNITIES AND CHALLENGES LA MONDIALISATION DE LA SANTÉ MENTALE 21 « La santé mentale globale au 21e siècle : Une plateforme catalytique l’innovation et la coopération transdisciplinaire » MENTAL HEALTH GOES GLOBAL: FROM GLOBALIZATION TO GLOBAL MENTAL HEALTH “21st Century Global Mental Health: A Catalytic Platform for Innovation & Transdisciplinary Collaboration”
- 3. 3 LEJOURNALDEL’AMPQ•DÉCEMBRE2017 3 CONTINUED »SUITE » I recently took part in a study conducted by Duke University in North Carolina aimed at preventing burnout among physicians. Although it may not be a diagnosis listed in the DSM, there is still both literature associated with and criteria that define burnout: fatigue, emotional exhaustion, cynicism related to your work and a sense of being unfulfilled, ineffective or not useful in your work. A study conducted in the United States reported that 30% of physicians suffer from burnout. With all of the upheavals and cutbacks that we have been experiencing over the last two years, it’s a fair bet that a Quebec study would probably reveal a rate twice as high. In light of this, I will divide this column into three parts: • Alerting you to the traps in our work environments that can contribute to burnout; • Highlighting the good the AMPQ is doing; and • Sharing some tricks that I have picked up with respect to resiliency. TRAPS BILL 130: DON’T SIGN ANYTHING! Bill 130 has been passed, and throughout the network, administrators are rushing to use their new powers, and even taking the opportunity to invent new ones. The beauty of the «Barrette plan» is that he appoints all of the managers, and once they are in position, they will have to do what he wants if they wish to keep their jobs. This provides him with scapegoats whom he can blame as his cutbacks ravage the network. The man is decidedly brilliant! You received my Psy Express by e-mail on November 27, 2017. Without rehashing everything here, I would like to remind you to remain vigilant, and to keep your- selves informed. You may be told that you are required to sign a contract in order to renew your privileges, but that is not the legal opinion of the FMSQ. On the contrary, the Federation strongly advises you to consult them before signing any document that could change your obligations and privileges. Billing details I often receive questions related to disputes with the RAMQ. We also submit requests for corrections or clarifications related to the definitions of service codes. Here are some suggestions to prevent the RAMQ from being able to recover payouts upon investigation, as much as possible: 1) Be sure to bill for your services within 90 days. After that, the RAMQ is within its right to not pay you, even if you have provided the services. The Régie can (but is not obliged to) extend this deadline, on an exceptional basis, if the professional demonstrates that it was impossible to act sooner. 2) The explanatory note related to billing for file reviews has been changed to provide a clearer reflection of what had been negotiated. Therefore, in cases where there is an extensive psychiatric history or numerous multidisciplinary assess- ments, the reviewing of a patient’s chart with addition of a summarizing note can be billed once per patient per physician per calendar year. It can be billed within ten working days preceding or following a medical examination. 3) The service code for review of the results of an analysis or examination is to be used for reviews of laboratory analyses or medical imaging. It is not to be used as a substitute for reviewing of reports prepared by other healthcare profes- sionals. It does not require the patient’s presence, rather it is done with the file. Récemment, j’ai participé à une étude de l’Université Duke de la Caroline du Nord visant à prévenir le burnout chez les médecins. Sans être un diagnostic DSM, le burnout a tout de même une littérature associée et des critères définis : la fatigue, l’épuisement émotionnel, le cynisme par rapport au travail, l’impression de ne pas s’accomplir, de ne pas être efficace ou utile dans son travail. Une étude américaine rapporte que 30 % des médecins sont en burnout. D’ailleurs, avec tous les cham- boulements et les compressions que nous vivons depuis deux ans, il est fort à pa- rier qu’une étude québécoise révèlerait sûrement des taux deux fois plus élevés. Ainsi, je vous présenterai cette chronique en trois temps : • pour vous mettre en garde contre les pièges qui se tendent dans nos milieux de travail pouvant contribuer au burnout ; • sur les réalisations de l’AMPQ ; et • un partage de trucs que j’ai appris sur la résilience. LES PIÈGES LOI 130 : NE SIGNEZ RIEN ! La 130 est passée et, partout dans le réseau, les administrateurs s’empressent d’utiliser leurs nouveaux pouvoirs et en profitent même pour s’en inventer. La beauté du « plan Barrette » c’est qu’il nomme tous les dirigeants qui, une fois en place, devront faire selon son souhait, sous peine de perdre leur poste. De plus, il s’est trouvé des boucs émissaires qu’il peut blâmer au fur et à mesure que ses compressions font des ravages dans le réseau. L’homme est décidément brillant ! Le 27 novembre dernier, vous receviez mon Psy Express par courriel. Sans tout reprendre ici, je vous rappellerai de demeurer très vigilants et de vous renseigner. Il se peut que l’on vous dise que vous êtes obligés de signer un contrat pour renou- veler vos privilèges, mais ce n’est pas l’avis juridique de la FMSQ. Au contraire, la Fédération vous suggère fortement de ne signer aucun document qui aurait pour effet de modifier vos obligations et vos privilèges sans vérifier au préalable avec eux. Précisions de facturation Régulièrement, je reçois des demandes relatives à des différends avec la RAMQ. De plus, nous faisons des demandes de corrections ou de précisions des défi- nitions des codes d’actes. Ci-après, certaines suggestions afin d’éviter le plus possible que la RAMQ soit en mesure de récupérer des sommes après enquête : 1) Assurez-vous de facturer vos actes à l’intérieur d’un délai de 90 jours. Par la suite, la RAMQ est en droit de ne pas vous payer, même si vous avez rendu les services. La Régie peut (ne doit pas mais peut) exceptionnellement prolonger ce délai si le professionnel démontre qu’il a été dans l’impossibilité d’agir plus tôt. 2) La note explicative sur la facturation de la révision de dossier a été modifiée afin de refléter plus clairement ce qui avait été négocié. Ainsi, dans le cas de lourds antécédents psychiatriques ou de nombreuses évaluations multidisciplinaires, la révision de dossier d’un patient comporte une note au dossier et peut-être factu- rée une fois par patient par médecin par année civile. Elle peut être facturée dans les dix jours ouvrables précédant ou suivant une visite. 3) L’acte de révision de résultats d’analyse ou d’examen, doit être utilisé pour les révisions d’analyses de laboratoire ou d’imagerie médicale. Il ne doit pas servir de substitut pour la révision de rapports rédigés par d’autres professionnels de la MOT DE LA PRÉSIDENTE MESSAGE FROM THE PRESIDENT Karine J. Igartua, M.D.
- 4. 4 LEJOURNALDEL’AMPQ•DÉCEMBRE2017 4 The purpose is to initiate, modify or maintain a course of treatment. Therefore, a change in dosage or medication is not required in order to bill under the code, but the examination that is requested and reviewed must be carried out in connection with the clinical decision about the treatment. 4) Beware of the temptation to make incorrect use of the codes for “medicaments d’exception” in order to have the RAMQ reimburse the cost of first-line agents. In the case of some long-acting injectables, the RAMQ only pays if the prescri- bing physician indicates code SN94 (compliance problem) or SN95 (conventional injectable antipsychotic ineffective or poorly tolerated). These codes necessarily imply that another drug (either an oral antipsychotic or a conventional injectable) has been tried previously. The same applies to long-acting stimulants. It is neces- sary to indicate that the rapid-acting stimulant has not provided adequate control (code SN132 for adults or SN103 for children). From a clinical perspective, this is frustrating when the practice guidelines recommend first-line use of extended release agents. Be aware that we are lobbying the government to change the status of these drugs, so as to be in keeping with the the guidelines. However, as long as these molecules continue to be categorized as “medicaments d’excep- tion”, physicians who use these codes improperly expose themselves to rather hefty fines. The improvement of its IT tools makes the RAMQ better able to detect the erroneous or fraudulent use of these codes. 5) Given the history of the negotiating strategy when the service codes were adopted, all of the medico-legal service codes that were negotiated within the framework of LE 172 exclude the concomitant use of the billing codes for follow- up interventions (“interventions de suivi - IS”) or third-party interviews (“entrevue de tiers – ET”). For example, if a psychiatrist meets with the family of a patient to collect a collateral history in order to be able to assess whether the patient represents a risk to himself or others, and whether a “garde en établissement” is necessary, these third-party interviews (ET) cannot be billed together with the fee for confinement assessment (98001). Similarly, if a psychiatrist discusses the behaviours observed since a patient’s arrival in the institution with the team to document his level of danger, these follow-up interventions are also non-billable. However, a loophole has opened up at the RAMQ. If your ET or IS is not related to the medico-legal assessment, and you can demonstrate that it was conducted in a separate session, then these acts would be payable. For example, if you place a patient under confinement in the morning, and then you discuss the drug treatment with the nurse in the evening, you could bill the IS. 6) It is possible to bill a patient for a missed appointment. Under CMQ rules, fees can be charged if the policy is posted and was mentioned at the time when the appointment was made, and the patient cancels within 24 hours of the appoint- ment. You will find four posters in this issue related to this: a. A document for your exclusive use, which indicates fees for services that are not insured by the RAMQ and those billed entirely outside of the RAMQ framework; b. Three posters to be displayed in waiting rooms: i. Services not insured by the RAMQ; ii. The notice to families of patients assessed by a psychiatrist; and iii. The policy respecting missed appointments. THE GOOD NEWS New administrators Following the resignations of the administrators from the Estrie and Saguenay Lac Saint-Jean regions, a nomination process was announced. A single application was received in each case. Therefore, Dr. Laurent Coulloudon (Saguenay Lac Saint-Jean region) and Dr. Patrick Lapierre (Estrie region) were appointed by acclamation as new administrators on the AMPQ Board of Directors. The mem- bers of the Board join me in welcoming them. Their dynamism and dedication are already evident. CANNABIS: we have been heard! The government has tabled its bill, and the news is rather good. Our efforts have borne fruit! Our ultimate goals were to ensure that legalization would not lead to increased cannabis use, that screening for psychotic episodes and dependency would go hand in hand with sales and that detoxification resources and First Episode Psychosis teams would be increased. We issued ten recommendations, focusing on the parameters of distribution and marketing, the establishment of an educational program addressing the risks of drug use and the consolidation of mental health resources for treating dependencies and psychoses. santé. Il doit se faire au vu du dossier. Il vise à initier, modifier ou maintenir un trai- tement. Un changement de posologie ou de molécule n’est donc pas requis pour facturer le code mais l’examen demandé et révisé doit être en lien avec la décision clinique par rapport au traitement. 4) Attention à la tentation d’utilisation erronée des codes pour les médicaments d’exception, afin que la RAMQ rembourse le cout des médicaments utilisés en première intention. Certains injectables à longue action ne sont payés par la RAMQ que si le prescripteur indique le code SN94 (problème d’observance) ou SN95 (antipsychotique injectable conventionnel inefficace ou mal toléré). Ces codes impliquent nécessairement qu’un autre médicament (soit un antipsychotique oral ou un injectable conventionnel) ait été essayé au préalable. Il en est de même pour les stimulants à action prolongée. Il faut indiquer que le stimulant à courte action n’a pas permis un contrôle adéquat (code SN132 pour les adultes, ou SN103 pour les enfants). Cliniquement, cela est frustrant lorsque les guides de pratique suggèrent les longues actions en première intention. Sachez que nous faisons du lobbying auprès du gouvernement pour changer le statut de ces médicaments afin de les rendre conformes aux lignes directrices. Cependant, tant que ces molécules demeurent des médicaments d’exception, le médecin qui utilise mal ces codes s’expose à des amendes assez sévères. Avec l’amélioration de ses outils infor- matiques, la RAMQ est davantage en mesure de déceler l’utilisation erronée ou frauduleuse de ces codes. 5) Compte tenu de l’historique de la stratégie de négociation lorsque les actes ont été mis en place, tous les codes d’actes médico-legaux négociés dans le cadre de la lettre d’entente 172 comportent l’exclusion de facturer avec ces actes des interventions de suivi ou d’entrevues auprès de tiers. Par exemple, lorsque le médecin psychiatre s’entretient avec la famille d’un patient afin d’avoir l’histoire collatérale pour lui permettre d’évaluer si le patient représente un risque pour lui- même ou les autres et si une garde en établissement est nécessaire, ces entretiens de tiers (ET) ne sont pas facturables en sus du tarif pour l’évaluation de la garde (98001). De même, lorsque l’on discute avec l’équipe des comportements obser- vés depuis l’arrivée d’un patient dans l’établissement, ces interventions de suivi (IS) ne sont également pas facturables. Par ailleurs, une brèche s’est ouverte à la RAMQ. En effet, si vos ET ou IS ne sont pas en lien avec l’évaluation médico-légale et que vous pouvez démontrer que cela s’est fait en séance différente, alors les ET et IS seraient payables. Par exemple, si vous mettez un patient sous garde le matin et qu’en soirée vous discutez de la pharmacologie à préconiser avec l’infirmière, vous pourriez facturer l’IS. 6) Il est possible de facturer un patient pour un rendez-vous manqué. Conformé- ment au CMQ, des frais peuvent être réclamés si la politique est affichée et qu’elle a été mentionnée lors de la prise de rendez-vous et que le patient annule à moins de 24 heures d’avis. À cet effet, vous retrouverez dans ce journal quatre affiches : a. Un document réservé exclusivement à votre usage, qui donne des indications de tarifs pour les services non assurés par la RAMQ et ceux facturés entière- ment à l’extérieur du cadre de la RAMQ ; b. Trois cartons à afficher dans les salles d’attente : i. Les services non assurés par la RAMQ; ii. L’avis aux familles des patients évalués par un psychiatre ; et iii. La politique dans le cas de rendez-vous non-respecté. LE BON Nouveaux conseillers Suite aux démissions des conseillers des régions de l’Estrie et du Saguenay Lac Saint-Jean, un avis de mise en candidatures a été lancé. Dans les deux cas, nous avons reçu une candidature et ainsi, le Dr Laurent Coulloudon (région du Sague- nay Lac Saint-Jean) et le Dr Patrick Lapierre (région de l’Estrie) ont été acclamés et deviennent les deux nouveaux conseillers au sein du CA de l’AMPQ. Ainsi, les membres du CA se sont joints à moi pour leur souhaiter la bienvenue. Déjà, leur dynamisme et leur dévouement sont évidents. CANNABIS : nos efforts portent fruit ! Le gouvernement a déposé son projet de loi et les nouvelles sont plutôt bonnes. Nos efforts ont porté fruit ! Nos objectifs ultimes étaient de faire en sorte que l’utili- sation du cannabis n’augmente pas avec la légalisation, que le dépistage des épi- sodes psychotiques et de la dépendance soient jumelés avec la vente, et que les ressources de désintoxication et les équipes de premiers épisodes psychotiques soient bonifiées. Nous avons émis un mémoire avec dix recommandations ciblant l’encadrement de la distribution et de la mise en marché et la mise en place de programme d’éducation aux risques de la prise de dogue ainsi que des ressources en santé mentale pour traiter les dépendances et les psychoses. CONTINUED »SUITE »
- 5. 5 LEJOURNALDEL’AMPQ•DÉCEMBRE2017 5 Minister Charlebois seems to have taken our concerns seriously, and the great majority of our recommendations are in the Bill. In addition, the AMPQ has been invited to testify before a parliamentary committee in January. This will allow us to assist the government in improving the bill, and to submit our recommendations respecting the regulations to be drafted afterwards. In parallel with this, we have launched an awareness campaign related to the dangers of cannabis. Many of you have assisted by sharing our poster on social networks and displaying it in waiting rooms. Some of you have requested additional copies for the schools in your regions, while others have even made presentations in high schools to help educate young people with respect to the risks associated with cannabis use. The AMPQ will soon be making a Powerpoint presentation for use in giving workshops to adolescents available to every psychiatrist who wishes to contribute to this educational effort. We would like to thank Dr. Coulloudon, who is heading up this initiative. The AMPQ journal 2.0 You have in your hands the final paper edition of the AMPQ journal. Beginning in 2018, we will be making the switch to an electronic version, which can be distri buted more rapidly, because there will no longer be delays related to printing or mail-delivery, and which will offer greater portability by being readable on your com- puter, tablet or telephone. It will also be more interactive, because it will be possible to insert useful links; more environmentally-friendly, because no trees will have to be sacrificed; and of course, less expensive for the Association. An app similar to that used by La presse+ is being contemplated. Watch your e-mail for information about how to sign up. Obviously, the journal will continue to be accessible on our site, in the members’ only section. RESILIENCY Researchers at Duke University have developed some simple strategies for increasing resiliency. They are based on the premise that our brains are naturally programmed to spot danger and bad things, while good things generally go unnoticed. We only notice the squeaky wheel, and not the three others operating silently. We remember the criticism received from one patient, but take no note of the thanks from others. We notice when it’s too cold or too hot, but not when it’s just right, and so on. In light of this, the researchers propose the idea that, in order to prevent depression, we need only train our brain to notice good things. The intervention consists of writing down three good things that happened every night before going to bed, and thinking back on our role in the matter. After ten days, you will begin to enjoy the exercise, and will start to notice good things throughout the day. Another tactic that provides protection against running out of steam is admiration. Admiring the sun’s light shining on leaves that are still clinging to the bough, the kindness of a colleague, the dedication of a parent of one of our patients, our daughter’s determined nature, our son’s skill, the colouring of a snail’s shell, etc. When we admire something, we freeze time for a few moments and immerse our- selves in the present. By giving ourselves the impression of slowing down time, we take a break from our frantic pace. Finally, and very fitting for the holiday season: random acts of kindness. Giving with no reason at all, without thinking about it too much, boosts your morale. It can be as simple as helping a mother get her stroller up the stairs at the shopping centre, paying for the coffee of the person in line behind you, passing your parking pay station receipt on to the person who is taking your space, etc. Try it and see. I know that many of us psychiatrists give of our time more systematically. In order to spread the word about the volunteer work that is done by our members, we are planning to create a page on our website next year. It will be a forum for highligh ting the involvement of psychiatrists in their community and encouraging others to donate time or money to the causes that are dear to our hearts. During this holiday season, if you decide to donate your money to a charitable organization, consider organizations that work in the health field, and specifically mental health. Support those organizations that work with our patients. The AMPQ makes two annual donations in your name, one goes to the FFAPAMM at the national level over a three-year period, while the other goes to an organization with a more regional or local mission, this year being «Weekends champêtres» on Montreal’s South Shore. Finally, I wish you a happy holiday season filled with recuperation and relaxation. May your 2018 be filled with health, peace, love and joy. La Ministre Charlebois semble avoir pris au sérieux nos inquiétudes et la grande majorité de nos recommandations ont été retenues. De plus, l’AMPQ est invitée à témoigner en commission parlementaire en janvier. Cela nous permettra d’aider le gouvernement à bonifier le projet de loi et de donner nos recommandations pour les règlements à pondre par la suite. En parallèle, nous avons déployé une campagne de sensibilisation aux dangers du cannabis. Plusieurs d’entre vous nous ont d’ailleurs aidés en partageant notre poster sur des réseaux sociaux et en l’affichant dans les salles d’attente. Certains ont demandé des affiches supplémentaires pour les écoles de leur région, et d’autres ont même donné des conférences dans les écoles secondaires pour ai- der à éduquer les jeunes sur les risques associés à l’utilisation du cannabis. Sous peu, l’AMPQ mettra à la disposition de tout psychiatre qui veut contribuer à cet effort d’éducation, une série de diapositives à utiliser pour donner des ateliers aux adolescents. Nos remerciements au Dr Coulloudon qui chapeaute cette initiative. Le journal de l’AMPQ 2.0 Vous tenez entre vos mains la dernière version papier du journal de l’AMPQ. Dès 2018, nous passerons à une version électronique plus rapidement dispo- nible, puisqu’il n’y aura plus de délais d’impression ou de poste, plus portative, en sachant que vous pourrez la lire sur votre ordinateur, votre tablette ou votre téléphone, plus interactive puisqu’il sera possible d’insérer des liens utiles, plus écologique étant donné qu’aucun arbre ne sera abattu et, bien entendu, moins dispendieuse pour l’association. Une application telle La presse+ est envisagée. Surveillez vos courriels pour les instructions relatives à l’abonnement. Évidem- ment, le journal sera toujours disponible sur notre site dans la section sécurisée, sous l’onglet des affaires syndicales. LA RÉSILIENCE Des chercheurs de l’université Duke ont mis au point des stratégies simples pour augmenter la résilience. Ces derniers se basent sur la prémisse que nos cerveaux sont naturellement programmés pour remarquer le danger et le mauvais alors que le bon passe généralement inaperçu. On ne remarque que la roue qui grince et non les trois autres silencieuses. On retient la critique d’un patient et on ne prend pas acte des remerciements des autres. On remarque lorsqu’il fait trop froid ou trop chaud, on ne note pas quand on est juste bien… Ainsi, les chercheurs avancent qu’il suffit d’entraîner notre cerveau à remarquer le bon pour prévenir la dépression. L’intervention consiste à écrire, tous les soirs avant de se coucher, trois choses qui ont bien été et à réfléchir sur notre rôle dans l’événement. Au bout de dix jours, on y prend goût et on commence à remarquer le bon tout au long de la journée. Une autre tactique qui nous protège contre l’essoufflement c’est celle de l’admi- ration. Admirer la lumière du soleil sur les feuilles qui résistent encore à tomber, la gentillesse d’un collègue, le dévouement d’un parent d’un de nos patients, la détermination de notre fille, la prouesse de notre fils, les couleurs de la coquille de l’escargot. Lorsqu’on admire, on arrête le temps quelques instants et on s’im- merge dans l’instant présent. En nous donnant l’impression de ralentir le temps, nous prenons une pause de notre rythme effréné. Finalement, et très à-propos pour le temps des fêtes : les actes aléatoires de gentillesse. Lorsqu’on donne de façon tout à fait gratuite, sans trop réfléchir, cela remonte le moral. Ça peut être aussi simple que d’aider une maman à remonter sa poussette dans les marches du centre d’achats, payer le café à celui qui est derrière vous dans la file, refiler votre ticket de stationnement payé au prochain qui prendra votre place, etc. Essayez et vous verrez. Je sais que nous sommes plusieurs psychiatres à donner plus systématique- ment de notre temps. Afin de partager avec tous le bénévolat accompli par nos membres, nous comptons lancer l’an prochain une page sur notre site web. En fait, il s’agira d’un forum pour mettre en lumière l’implication des psychiatres dans leur communauté et encourager d’autres à donner temps ou argent aux causes que nous chérissons. En ce temps des fêtes, si vous décidez de donner votre argent à une œuvre de charité, pensez aux organismes qui travaillent en santé, et spécifiquement en santé mentale. Encouragez les organismes qui agissent auprès de nos patients. En votre nom, l’AMPQ fait deux dons annuels, l’un à portée nationale sur une période de trois ans, est remis à la FFAPAMM et l’autre, à un organisme dont la mission est plus régionale ou locale est attribué à « Weekends champêtres », de la Rive-Sud de Montréal. En terminant, je vous souhaite un joyeux temps des fêtes, ressourçant et repo- sant. Santé, sérénité, amour et joies en 2018.
- 6. ER chez les médecins du Québec ERER chez les médecinschez les médecins du Québec Médecins psychiatres, faites comme 5000 de vos collègues qui, chaque jour, nous font confiance pour leur facturation. Notre équipe de conseillers experts vous propose un accompagnement personnalisé basé sur la proximité, la collaboration et la transparence. Cette approche, combinée au logiciel de facturation médicale le plus utilisé au Québec, vous offre la tranquilité d’esprit dont vous avez besoin au quotidien. Mises à jour optimales des nouvelles normes Découvrez plus d’avantages en ligne au Facturation.net Clavardage en ligne accessible 24 /24 Analyse personnalisée pour optimiser vos revenus
- 7. 7 LEJOURNALDEL’AMPQ•DÉCEMBRE2017 7 Hello! As the photograph above can attest, Dr. Assalian has indeed retired as President of the Continuing Professional Develop- ment (CPD) Committee! On this occasion, I wish to join all those who have thanked him for his unwavering work during 12 years of service at the AMPQ during which he organized hundreds of CPD activities. Allow me to introduce myself: Richard Montoro, new Pre- sident of the CPD Committee since this September, psychia- trist at McGill University, specialized in mental health issues related to sexual orientation and gender identity. I’ve recently completed six years as Assistant Dean of Resident Profes- sional Affairs at McGill University, and in the same period, I was the FMSQ Board where I had the chance to be involved in the organizing committee of the JFI (Journée de formation interdis- ciplinaire), and the development of the Méduse platform. To recap, CPD at the AMPQ is doing very well. We’ve just received our Accreditation for the next eight years from the Royal College, along with congratulations from the review committee members who were impressed by the diversity and the quality of our offerings, such as lunchtime web- conferences, Friday seminars, and Weekend Pedagogical Retreats. Given such successes, should we say: “Rinse and Repeat”? Well, not quite. In July 2018, the Collège des médecins du Québec will introduce its new obligatory CPD activities, which will include self-assessment hours which are roughly equiva- lent to the Section 3 credits required by the Royal College. Thus, we’ll be working with our Méduse partners in the co- ming months to develop a diversity of content to meet all your CPD needs. Stay tuned! Worry not, the annual conference will remain our flagship event, and 2018 will be the stage for not one but two qua- lity AMPQ conferences! The 52nd Annual Conference will take place in Bastia, Corsica, on May 14–16, 2018, in collaboration with our French colleagues of the CPNLF Association. You’ll soon receive the scientific and social programs for this activity. We’ve also worked with the Caméléo agency to develop a week-long excursion to explore Corsica after the conference. When the annual conference takes place outside Canada, AMPQ holds a local “pre-conference”, which we’ve affec- tionately named Le Condensé. Indeed, the title refers to an abundance of various subjects, which we’ve condensed into two days. On April 19–20, you’ll have access to presenta- tions on electroconvulsive therapy, gerontopsychiatry, medi- colegal psychiatry, innovations in psychiatry, international guest speakers, and of course, Section 3 credits! Reserve these dates and watch your inbox for up-to-date information! Finally, our next CPD needs assessment survey will be launched in spring 2018. Meanwhile, don’t hesitate to contact me, the members of the CPD Committee or Caroline Piecha to share your ideas, your challenges and your needs in mat- ters of continuing development. It’s always a pleasure to receive suggestions for topics, lecturers and pedagogical innovations. I look forward to working with you and getting to know you through our AMPQ CPD activities! ampq.dpc@fmsq.org Chers lecteurs Vous avez sûrement déduit par la photo que le Dr Assalian a pris sa retraite de la présidence du DPC. J’en profite pour joindre ma voix à tous ceux et celles qui l’ont remercié pour son travail indéfectible pendant ses douze ans de service à l’AMPQ et pour l’organisation de plus d’une centaine d’activités de développement professionnel continu. Alors, permettez-moi de me présenter : Richard Montoro, nou- veau président du comité de DPC depuis septembre, psychiatre à l’Université McGill se spécialisant dans les difficultés reliées à l’orientation sexuelle et à l’identité de genre. J’ai récemment complété six ans comme vice-doyen adjoint aux affaires pro- fessionnelles des résidents à McGill, et parallèlement, six ans au conseil d’administration de la FMSQ, où j’ai eu la chance de m’impliquer dans le comité organisateur des JFI et dans le déve- loppement de la plateforme Méduse. Rappelons-nous que le DPC à l’AMPQ se porte très bien. Nous venons d’obtenir notre agrément du Collège royal pour huit ans avec les félicitations des membres du comité de révision qui ont été impressionnés par la diversité et la qualité de nos for- mats pédagogiques, tels les webconférences, les formations du vendredi et les week-ends pédagogiques. Doit-on utiliser l’expression anglaise « Rinse and repeat » ? Pas tout à fait. En juillet 2018, le CMQ déposera son projet de loi sur le DPC qui inclura une obligation d’effectuer des heures d’autoévaluation de la pratique. Ces heures seront l’équivalent des crédits de section 3 déjà requis par le Collège royal. Dans les prochains mois, nous travaillerons avec l’équipe de Méduse pour offrir un contenu diversifié afin de vous aider à répondre à ces critères. À suivre ! Ne craignez rien, notre congrès annuel restera notre événe- ment phare et 2018 nous réserve pas un, mais deux congrès AMPQ de qualité ! Le 52e congrès annuel se tiendra à Bastia, en Corse, du 14 au 16 mai 2018 avec nos collègues français de l’Association du CPNLF. Vous devriez recevoir sous peu la pro- grammation scientifique et sociale de cette activité. Nous avons également travaillé avec l’agence Caméléo pour développer un voyage d’extension d’une semaine afin de découvrir la Corse. Comme vous le savez, lorsque le congrès annuel est à l’exté- rieur du pays, l’AMPQ tient un « précongrès » local que nous avons surnommé affectueusement « Le Condensé ». En effet, le titre fait référence à l’abondance de sujets divers que nous avons condensés en deux jours. Les 19-20 avril prochain, vous aurez accès dans une même formation à de l’électroconvulsi- vothérapie, de la gérontopsychiatrie, du médicolégal, des inno- vations en psychiatrie, des conférenciers de renommée et bien sûr de la section 3 ! Réservez les dates et surveillez votre courrier pour tous les détails ! Et finalement, notre prochain sondage d’évaluation des besoins en DPC sera déployé au printemps 2018. En attendant, n’hési- tez surtout pas à communiquer avec moi, avec les membres du comité de DPC, ou avec Caroline Piecha afin de partager vos besoins, vos idées, vos défis ou même vos envies en DPC. Il nous fait toujours plaisir d’avoir des suggestions de sujets, de conférenciers ou d’innovations pédagogiques. Au plaisir de travailler avec vous et d’apprendre à vous connaître dans le cadre des formations de l’AMPQ. ampq.dpc@fmsq.org MOT DU PRÉSIDENT DU COMITÉ DE DÉVELOPPEMENT PROFESSIONNEL MESSAGE FROM THE PRESIDENT OF THE PROFESSIONNAL DEVELOPMENT COMMITTEE Richard Montoro, M.D.
- 8. SUITE » CONTINUED » Medical literature grows exponentially. In 2010, it was es- timated that the number of scientific papers in medicine doubled every 3.5 years, and by 2020, this number will be every 73 days.1 This impressive accumulation of know- ledge creates a significant challenge for the general psych- iatrist who must follow the rhythm to maintain his skills and improve care quality. The consultation-liaison (CL) practice is no stranger to this trend. This psychiatric spe- cialty, which focuses on psychiatric care for patients with a physical illness, is evolving as rapidly as ever. Recent data has changed our ways of seeing things in that do- main. Here are some examples: the studies on the impact of “intestine-brain communication” on psychiatric condi- tions 2 , the unclear risks/benefits ratio of the reliance on antipsychotics for delirium 3 , the important and often over- looked clinical elements in the evaluation of the aptitude to consent to care 4 , and the psychosocial issues, which can influence or motivate one’s own request for an early death in the event of a severe illness 5-8 , etc. It’s estimated that in Québec, close to 60 psychiatrists work either occasionally or full time on psychiatric consul- tation-liaison. Yet, in Canada and Québec, few organiza- tions offer continuing education in this field. That’s why the Société québécoise de consultation-liaison et de médecine psychosomatique proposed last June, at AMPQ’s annual congress, a symposium led by three psychiatrists special- izing in CL who accepted to share their most recent clinical pearls with their colleagues who may have to deal with CL. The SQCM presents here three articles, which summarize the outlines of the symposium through a question-answer formula with the three lecturers. The first article is entitled Delirium 201 by Dr. Nicolas Bergeron, the second will discuss the aptitude to consent to or to refuse a medical- surgical intervention, by Dr. Karl Looper, and the third will focus on mental suffering of the patient requesting medical assistance in dying (MAD), by Dr. Suzanne Leclair. Happy reading! La littérature médicale continue de croître de façon expo- nentielle. En 2010, on estimait que le nombre d’écrits scientifiques en médecine doublait tous les 3,5 ans, et dès 2020 tous les 73 jours 1 . Cette accumulation impres- sionnante de connaissances pose un défi de taille au psy- chiatre général qui doit suivre le rythme pour maintenir ses compétences afin d’offrir des soins de qualité. Et la consultation-liaison ne fait pas exception à cette réalité ! Cette spécialité psychiatrique qui s’intéresse aux soins psychiatriques adaptés aux patients atteints de maladie physique évolue aussi rapidement. De récentes données ont d’ailleurs changé notre façon de voir les choses. On pense notamment aux études sur l’impact de la « com- munication intestin-cerveau »(!) sur les affections psychia- triques 2 , au ratio pas si clair risques/bénéfices du recours aux antipsychotiques en cas de delirium 3 , aux éléments cliniques importants et souvent peu considérés lors de l’évaluation de l’aptitude à consentir aux soins 4 , aux pro- blématiques psychosociales qui peuvent influencer ou motiver les demandes de voir sa propre mort hâtée au cours d’une maladie grave 5-8 , etc. On estime, qu’au Québec, près d’une soixantaine de psychiatres consacrent en totalité ou partiellement leurs activités cliniques à la pratique de la psychiatrie de consul- tation-liaison (CL). Or, peu d’organisations offrent, tant au Québec qu’au Canada, une formation continue dans cette matière. C’est pourquoi la Société québécoise de consultation-liaison et de médecine psychosomatique proposait en juin dernier, dans le cadre du congrès annuel de l’AMPQ, un symposium réunissant 3 psychiatres spé- cialisés en CL qui avaient accepté de partager leurs plus récentes perles cliniques avec leurs collègues psychiatres qui ont une pratique générale ou en partie dédiée à la CL. La SQCM propose donc ici une série de trois articles résu- mant les grandes lignes de ce symposium grâce à une formule questions-réponses avec les trois conférenciers. Le premier article présenté ici traitera du delirium 201 avec Dr Nicolas Bergeron, le second portera sur l’aptitude à consentir ou à refuser des soins médico-chirurgicaux (en- trevue avec Dr Karl Looper), et le dernier, sur la souffrance psychique du patient demandant l’aide médicale à mourir (AMM) (entrevue avec Dre Suzanne Leclair). Bonne lecture ! POST-CONGRÈS 2017 POST-CONGRESS 2017 CONSULTATION-LIAISON : PETITS TRUCS FONDÉS SUR LES DONNÉES PROBANTES POUR LE PSYCHIATRE GÉNÉRAL QUI COURT TOUJOURS (1er article d’une série de 3) CONSULTATION-LIAISON: TIPS BASED ON CONCLUSIVE DATA FOR THE PSYCHIATRIST ON THE RUN (first of a three-part series) Jacynthe Rivest, M.D. Présidente, SQCM (Société québécoise de consultation-liaison et de médecine psychosomatique) President, SQCM (Société québécoise de consultation-liaison et de médecine psychosomatique) Nicolas Bergeron,M.D. Médecin psychiatre spécialisé en consultation-liaison, CHUM, et chercheur investigateur, CRCHUM Psychiatrist specialized in consultation-liaison, CHUM, and researcher, CRCHUM LEJOURNALDEL’AMPQ•DÉCEMBRE2017 8
- 9. 9 LEJOURNALDEL’AMPQ•DÉCEMBRE2017 9 CONTINUED »SUITE » DELIRIUM 201 – INTERVIEW WITH DR. NICOLAS BERGERON Psychiatrist specialized in consultation-liaison, CHUM, and researcher, CRCHUM CRCHUM JR: The publication of the DSM-5 was the perfect occasion to edit the diagnostic criteria of several men- tal disorders. Any changes for delirium? A little, and mostly in the English version. In French, the first criterion still mentions a perturbation of the attention and the consciousness, but in English, we read: disturbance in attention and awareness. So, in a way, that version does away with the level of consciousness, and refers mostly to awareness. It also specifies the fact that delirium cannot be considered within the context of a highly reduced level of awareness (such as is the case in a comatose or stupor- ous state). Although delirium can be linked to drowsiness, there’s a difference between being sleepy (such as a side effect of a painkiller), and not being fully aware of what’s happening around us for a while. JR: Consciousness isn’t easy to measure. How can we evaluate it at a patient’s beside? Consciousness is the mental ability, which allows us to subjectively grasp exterior or interior phenomena and, more generally, our own existence. When we ask a person about the date and place where he is, we’re not interested in his memory capacities as much as about how he ori- ents himself in his environment, and how he perceives time and passing events. We can interrogate that person on his health status, on past or future interventions, on a room change, or the visit of family. In short, anything that might help know if the person is with us or in the woods. To check on a person’s capacity for attention, over and above his capacity to follow the conversation, we can use short objective cognitive tests such as naming months in the reverse order, spell his name backwards, squeeze fingers whenever the letter a is pronounced such as in spelling “abracadabra”. Drawing a clock is also quite revealing on the state of executive and visuospatial functions of the per- son examined. JR: When taking care of a person with delirium, we know that we must first treat associated medical con- ditions such as hypoxemia, infection, dehydration, and stop, if possible, medication that could be pot- entially delirium-provoking such as opioids, benzodi- azepines, tricyclics; however, we often prescribe an antipsychotic almost as a reflex. Can we continue this practice in the light of conclusive data? What’s amazing is that haloperidol, considered as the gold standard in the pharmacological treatment of delirium, has never been submitted to a placebo-controlled trial. None. The strong historical conviction that this medication was very good may have shied away ethics committees. The last systematic reviews and meta-analysis indexed fewer than 12 randomized and controlled studies (only, and for a syndrome, which affects 20% of the population of a hos- pital). The conclusion is that there’s no evidence indicating that an antipsychotic lessens the length of delirium. In some studies, a more rapid resolution of the severity of the case is observed, but it’s not too impressive. However, in the day- to-day life, we don’t hesitate to prescribe an antipsychotic to control agitation or to help with a psychosis associated DÉLIRIUM 201 – ENTREVUE AVEC DR NICOLAS BERGERON Médecin psychiatre spécialisé en consultation-liaison, CHUM, et chercheur investigateur, CRCHUM JR : La venue du DSM-5 a été l’occasion de revisiter les critères diagnostiques de nombreux troubles mentaux, est-ce qu’il y a eu du changement pour le délirium ? « Un peu, et en fait, surtout dans la version anglaise. En français, le 1er critère mentionne toujours une perturbation de l’attention et de la conscience mais en anglais, on a préféré disturbance in attention and awareness (plutôt que consciousness). On se détache d’une certaine façon du niveau de conscience qui fait davantage référence à la vigi- lance. On a aussi tenu à préciser que le délirium ne pouvait être considéré dans le contexte d’un niveau de vigilance très réduit (comme dans un état comateux ou stuporeux). Le délirium peut être associé à de la somnolence mais il y a une différence entre être endormi (souvent après la prise d’un analgésique) et ne pas trop savoir ce qui se passe autour de soi pour un certain temps. » JR : La conscience ou la prise de conscience n’est pas facile à mesurer, quelles seraient les façons de l’éva- luer au chevet d’un malade ? «Laconscience,c’estlafacultémentalequipermetd’appré hender de façon subjective les phénomènes extérieurs ou intérieurs et, plus généralement, sa propre existence. Lorsque l’on demande la date ou l’endroit où se trouve une personne, on ne s’intéresse pas tant à ses capacités mné- siques mais à comment elle s’oriente dans son environne- ment et comment elle perçoit le temps et les événements qui passent. Ensuite, on peut l’interroger sur son état de santé, les interventions reçues ou à venir, un changement de chambre ou une visite d’un proche. En bref, tout ce qui permet d’apprécier si la personne est avec nous ou au contraire, un peu à côté de la track. Pour l’attention, en plus d’apprécier si la personne suit bien la conversation, il est intéressant d’utiliser de courts tests cognitifs objectifs comme nommer les mois à rebours, épeler son nom à l’envers, serrer nos doigts lorsque l’on prononce la lettre « A » en épelant « ABRACADABRA ». Le dessin d’une hor- loge est aussi fort révélateur sur les fonctions exécutives et visuospatiales de la personne examinée. » JR : Dans la prise en charge d’un patient avec un déli- rium, on sait que l’on doit d’abord traiter les affections médicales associées (hypoxémie, infection, déshy- dratation) ou retirer si c’est possible des médicaments potentiellement déliriogéniques (opiacés, benzodia- zépines, tricycliques) mais on a souvent le réflexe d’ajouter d’emblée un antipsychotique. Cette pratique est-elle encore soutenue par les données probantes ? « Ce qui est fort étonnant, c’est que l’halopéridol, considéré comme le médicament étalon-or (le gold standard) dans le traitement pharmacologique du délirium n’a jamais fait l’ob- jet d’une étude contre placebo. Aucune. La conviction his- torique que ce médicament était très bon a peut-être rendu frileux les comités d’éthique. Les dernières revues systéma- tiques et méta-analyses répertorient moins de 12 études randomisées et contrôlés (seulement ! pour un syndrome dont la prévalence avoisine le 20 % dans un hôpital). La conclusion : aucune évidence qu’un antipsychotique dimi- nue la durée du délirium. Dans quelques études, on observe L’ENREGISTREMENT VIDÉO DE LA PRÉSENTATION EST DISPONIBLE SUR LA PLATEFORME MÉDUSE DE LA FMSQ. THE VIDEO RECORDING OF THE INTERVIEW CAN BE SEEN ON FMSQ’S MEDUSA PLATFORM.
- 10. 10 LEJOURNALDEL’AMPQ•DÉCEMBRE2017 10 with delirium. This practice is appropriate. Some studies targeting more specific symptoms or high-risk populations would be welcome. We must say that research on delirium is far from easy. Just think about the question of consent and the state of instability associated with delirium. JR: And what about the often-mentioned non-phar- macological interventions (psycho-environmental)? Do they work? Multi-component programs include many targeted inter- ventions such as hydration, pain control, review of medica- tion, sleep facilitation (without benzodiazepine, to prohibit, don’t forget), the mobilization, the stimulation, the reorien- tation, the correction of sensory deficits, and education (of both family and personnel). These programs clearly decrease the incidence of delirium – quite impressive for measures that are often viewed as inferior to antipsychot- ics. On the other hand, their efficiency is not as obvious in the case of a person with dementia. Obviously, we can’t establish all this instantly. Our role for now, as psychiatrists, along with geriatric services, will be to encourage the care teams to setup simple measures with an important impact on the quality of care. Continued in the next journal… REFERENCES 1. Freudenreich, O., et al., Updates in Psychosomatic Medicine: 2014. Psychosomatics, 2015. 56(5): p. 445-59. 2. Mason, B.L., Feeding Systems and the Gut Microbiome: Gut-Brain Interactions With Relevance to Psychiatric Conditions. Psychosomatics, 2017. 3. Thom, R.P., C.K. Mock, and P. Teslyar, Delirium in hospitalized patients: Risks and benefits of antipsychotics. Cleve Clin J Med, 2017. 84(8): p. 616-622. 4. Kontos, N., J. Querques, and O. Freudenreich, Capable of more: some underemphasized aspects of capacity assessment. Psychosomatics, 2015. 56(3): p. 217-26. 5. Bellido-Pérez, M., et al., Assessment of the wish to hasten death in patients with advanced disease: A systematic review of measurement instruments. Palliat Med, 2017. 31(6): p. 510-525. 6. Guerrero-Torrelles, M., et al., Meaning in life as a mediator between phy- sical impairment and the wish to hasten death in patients with advanced cancer. J Pain Symptom Manage, 2017. 7. Robinson, S., et al., The Relationship Between Poor Quality of Life and Desire to Hasten Death: A Multiple Mediation Model Examining the Contributions of Depression, Demoralization, Loss of Control, and Low Self-worth. J Pain Symptom Manage, 2017. 53(2): p. 243-249. 8. Rodriguez-Prat, A., et al., Understanding patients’ experiences of the wish to hasten death: an updated and expanded systematic review and meta-ethnography. BMJ Open, 2017. 7(9): p. e016659. une résolution plus rapide de la gravité mais ce n’est pas très impressionnant. Toutefois, dans la vie de tous les jours, on n’hésitera pas à donner un antipsychotique pour contrôler une agitation ou soulager une psychose associée à un délirium. Cette pratique est appropriée. Des études ciblant des symptômes plus spécifiques ou sur des populations à haut risque seraient le bienvenu. On doit dire que la recherche sur le délirium n’est pas facile. Pensez juste au consentement et l’instabilité de l’état de santé associée. » JR : Et les interventions dites non-pharmacologiques (psycho-environnementales) souvent citées sont-elles efficaces ? « Des programmes dits à composantes multiples incluent plusieurs interventions ciblées comme l’hydratation, le contrôle de la douleur, la révision de la médication, la facilitation du sommeil (sans benzodiazépine ! à proscrire, ne l’oublions pas), la mobilisation, la stimulation, la réorientation, la correction des déficits sensoriels et l’éducation (des proches et du personnel aussi). Or, ces programmes diminuent clairement l’incidence du délirium. C’est très impressionnant pour des mesures moins souvent considérées que les antipsychotiques. En revanche, l’effet n’est pas aussi certain pour les personnes avec une démence. Évidemment, on ne peut mettre cela en place sur une garde… Notre rôle de psychiatre, en s’associant avec la gériatrie, sera d’encourager les équipes soignantes à mettre en place des mesures simples mais dont l’impact sera important sur la qualité des soins. » La suite, dans le prochain journal… RÉFÉRENCES 1. Freudenreich, O., et al., Updates in Psychosomatic Medicine: 2014. Psychosomatics, 2015. 56(5): p. 445-59. 2. Mason, B.L., Feeding Systems and the Gut Microbiome: Gut-Brain Interactions With Relevance to Psychiatric Conditions. Psychosomatics, 2017. 3. Thom, R.P., C.K. Mock, and P. Teslyar, Delirium in hospitalized patients: Risks and benefits of antipsychotics. Cleve Clin J Med, 2017. 84(8): p. 616-622. 4. Kontos, N., J. Querques, and O. Freudenreich, Capable of more: some underemphasized aspects of capacity assessment. Psychosomatics, 2015. 56(3): p. 217-26. 5. Bellido-Pérez, M., et al., Assessment of the wish to hasten death in patients with advanced disease: A systematic review of measurement instruments. Palliat Med, 2017. 31(6): p. 510-525. 6. Guerrero-Torrelles, M., et al., Meaning in life as a mediator between phy- sical impairment and the wish to hasten death in patients with advanced cancer. J Pain Symptom Manage, 2017. 7. Robinson, S., et al., The Relationship Between Poor Quality of Life and Desire to Hasten Death: A Multiple Mediation Model Examining the Contributions of Depression, Demoralization, Loss of Control, and Low Self-worth. J Pain Symptom Manage, 2017. 53(2): p. 243-249. 8. Rodriguez-Prat, A., et al., Understanding patients’ experiences of the wish to hasten death: an updated and expanded systematic review and meta-ethnography. BMJ Open, 2017. 7(9): p. e016659. Date limite de soumission : 16 février 2018 Détails et formulaires disponibles sur www.ampq.org sous l’onglet Prix annuels de l’AMPQ 2018 Pour plus d’informations, communiquez avec Johanne Meunier au 514 350-5128
- 11. SUITE » CONTINUED » 11 LEJOURNALDEL’AMPQ•DÉCEMBRE2017 11 As our ironic title suggests, the current debate on the legalization of cannabis in Quebec is somewhat weari- some for our association. Since the beginning of discus- sions on the subject, I hear my colleagues say: “This is beyond comprehension,” or “our patients are already talk- ing about Mr. Trudeau’s legal cannabis,” or “the young will consume more,” or “the winds of banalization will blow over Quebec.” However, I tell myself that there must be sound reasons for this C-45 Federal Bill, a bomb ticking until July 2018. No one yet knows what will happen follow- ing that date once this huge project comes into effect. In the meantime, opinions ring out in all directions, and feed the discussion. A few weeks ago, motivated by deep beliefs, I decided to get involved in AMPQ’s awareness campaign, and defend the position of Quebec psychiatrists on the legalization of cannabis. Along with several colleagues, I participated in TV and radio interviews—a gratifying experience, which helped me discover the extent to which Quebecers ignored the facts surrounding the risks of cannabis use. Many persons requested more information on the subject and, among others, a high-school worker on substance abuse who invited me to deliver a conference at her insti- tution. After this first conference, I realized how keenly inter- ested young people were in this subject, and knowing how crucial this issue was, I decided to tour the schools of my region. I never thought I’d have the time to do that, given my clin- ical timetable. Of course, I’ve often discussed privately with each of my patients about the risks of cannabis use. I found, however, that it was far more cost-effective in terms of time to address 160 young people at once. When the doctor speaks, young people listen. We have a level of credibility shared by few in the medical and social systems. With respect to cannabis, I’m not on a fear propaganda crusade: I explain the reasons why we legalize cannabis (still little info on that): electoral campaign promise, decrim- inalization of simple possession, occasion to control the quality of the substance, the wish to stop black market practises, etc. I also explain what the risks of cannabis use are (and some other drugs too), while stressing how to reduce the harmful effects of cannabis consumption. “If you decide to use cannabis, be aware of how you do it, of the quantity used, and of THC concentration.” In my lectures, I also mention school problems in general as related to cannabis, and I mention the fact that many young people who have ADHD actively use cannabis be- cause their usual psycho stimulating medication may not be as effective, and that is one area where cannabis can Je me permets le jeu de mot, il est facile. Les derniers mois furent éprouvants pour notre association dans le cadre des débats sur la légalisation du cannabis au Québec. Depuis le tout début, j’entends mes collègues me dire que cela n’a pas de bon sens, que nos patients nous parlent déjà du cannabis légal de Monsieur Justin Trudeau, que les jeunes vont davantage consommer, qu’il soufflera un vent de banalisation du cannabis au Québec. Je réfléchis, et je me dis qu’il doit bien y avoir une bonne raison pour ce projet de loi fédéral C-45, parachuté comme une bombe avec une minuterie qui fait tic-tac jusqu’en juillet 2018 (ou avant ?). Que va-t-il réellement se passer après la légalisation ? Avec un projet d’une telle envergure dans un pays comme le Canada, personne ne le sait. Mais tout le monde a son opinion, et c’est ce qui est intéressant. Par conviction, dans les dernières semaines, j’ai eu la chance d’être impliqué activement dans la campagne publicitaire de l’AMPQ afin de défendre la position des psychiatres québécois sur la légalisation du cannabis. J’ai donné plusieurs entrevues à la radio et à la télévision, comme plusieurs de nos collègues. Cette expérience fut extrêmement enrichissante, car elle m’a permis de constater à quel point la population québécoise était peu informée face aux risques reliés à la consommation de cannabis. Plusieurs personnes m’ont interpellé afin d’avoir davantage d’informations sur le sujet, dont une intervenante en toxicomanie dans une école secondaire qui m’a invité à venir donner une conférence. J’ai accepté. Après une première conférence, en voyant l’intérêt des jeunes, je me suis dit qu’il faudrait faire le tour des écoles de notre région. L’enjeu est beaucoup trop important. Pour être franc, je n’aurais jamais pensé faire de la prévention primaire à travers toute ma charge clinique, mais en y pensant bien, cela fait du sens. Je passe tellement de temps à discuter avec les patients, un par un, des dangers du cannabis, que de le faire devant 160 jeunes rentabilise mon temps au maximum. Et quand le docteur parle, les jeunes écoutent. Nous avons une autorité que peu d’intervenant dans notre système médical ou social possède. Je ne fais pas une « campagne de peur » sur le cannabis, j’explique aux jeunes pourquoi il y aura une légalisation du cannabis (car personne ne leur a encore expliqué...) ; promesse électorale, décriminalisation de la possession, opportunité de contrôler la qualité de ce qui circule, souhait d’enrayer le marché noir, etc. Je leur explique aussi quels sont les risques reliés à la consommation de cannabis (et un peu des autres drogues), tout en discutant d’une approche par la réduction des méfaits (ex. : si jamais vous décidez de consommer du cannabis, faites attention au mode de consommation, à la quantité, et au niveau de THC.). Je touche aussi le sujet des difficultés scolaires de façon générale, en abordant le fait que certains jeunes souffrant de TDAH consomme activement du cannabis ; il peut arriver Laurent Coulloudon, M.D. UN DÉBAT FUMANT A FUMING DEBATE
- 12. 12 LEJOURNALDEL’AMPQ•DÉCEMBRE2017 12 become a significant factor of confusion. Overall, I know that young people have many questions on this subject. My active involvement in this debate also showed me the other side of the coin. Indeed, I’ve received several comments from health workers and researchers in sub- stance abuse who characterized my approach and that of AMPQ’s as dangerous, prohibitive, and alarming. Because I’m not a public health expert, I started reading on this position seemingly diametrically opposite to ours, and I realized how important it was to consider all points of view. Indeed, the prohibitive approach has limits, as we see every day in our clinics. How many patients in our clinical work are on probation or supervised in some capacity by a tribunal, and who still use cannabis despite their situation. Moreover, making consumption illegal for persons 18–21 years of age (the age group most prone to cannabis use) could have the opposite effect, pushing them toward the black market, thus defeating the whole concept of legal- ization. These young people would become criminalized in increasing numbers, thus bogging down our justice system. Finally, the simple fact of informing our patients on the risks of cannabis use, will not necessarily lead to abuse cessa- tion. So, now that we’ll be able to control both the quality of the substance and the THC concentration, we will have to make sustained efforts over the years to reduce the harm done to our substance abuse patients. While I’m writing these lines, the provincial government still hasn’t proposed a draft legislation for the legalization of cannabis. Let’s hope that even if cannabis is available to those from 18 years of age, the government will keenly listen to our recommendations concerning education on the risks of cannabis use, the risk of banalization, the need to identify problematic consumers, and the necessity to provide all possible resources in psychiatry and substance abuse, to make sure they are in place, ready to deal with the consequences of cannabis legalization. Whatever the outcome, I think that the credibility linked to our profession, and to our association gives us a privilege on the public stage in Quebec, and allows us to improve prevention and the development of awareness on the use of cannabis. Only then do we have a chance to prevent legalization from becoming banalization. Let’s make sure the train doesn’t derail. que ces jeunes se plaignent que leur médication psycho stimulante est sous-optimale, alors que le cannabis est un facteur confondant important. Je me rends compte que les jeunes ont plusieurs questions pertinentes sur tous ces sujets. Mon implication dans ce débat m’a permis aussi de voir un autre côté de la médaille. En effet, j’ai reçu des cri- tiques de certains intervenants ou chercheurs en toxico- manie qui qualifiaient mon approche, et celle de l’AMPQ, de « dangereuse », de « prohibitive », d’une approche alarmiste pour la population. N’étant pas un spécialiste de la santé publique, je me suis mis à lire sur cette autre position qui est quelquefois présentées comme étant dia- métralement opposée à la nôtre, pour me rendre compte qu’il y avait plusieurs points à considérer. Effectivement, l’approche prohibitive a ses limites, comme nous le voyons tous les jours en clinique. Combien de patients avez-vous dans votre charge clinique qui sont encadrés par une pro- bation ou par le TAQ, et qui fument activement du canna- bis malgré leurs conditions ? Par ailleurs, le fait d’interdire la vente à la population de 18 à 21 ans (la tranche d’âge ayant la plus grande prévalence de consommation de can- nabis) pourrait ne pas avoir l’effet escompté de diminuer la prévalence de consommation chez cette population. D’autant plus, ces jeunes de 18 à 21 ans risque de conti- nuer à s’approvisionner en cannabis sur le marché noir, ce qui viendrait à l’encontre des l’objectifs de réduction des méfaits de ce projet de loi. Ces jeunes seraient aussi davantage criminalisés, embourbant notre système de jus- tice. Finalement, le simple fait de parler des dangers aux patients ne fera pas toujours en sorte qu’ils vont cesser de consommer ; peut-être faudra-t-il davantage aborder dans les prochaines années la réduction des méfaits avec nos patients consommateurs maintenant que nous pouvons contrôler la qualité de la drogue consommée et choisir un niveau de THC ? Au moment d’écrire ces lignes, le gouvernement provin- cial n’a pas encore dévoilé son projet de loi pour encadrer la légalisation. Espérons que même s’il légalise la vente à partir de 18 ans, il retiendra nos autres recommandations qui visent toutes à éduquer sur les risques de la consom- mation, contrer la banalisation, dépister les consomma- teurs problématiques, et s’assurer que les ressources en psychiatrie et en toxicomanie sont au rendez-vous. Peu importe l’issu final, je crois que notre autorité et notre cré- dibilité sur la place publique, en tant qu’association, nous permettront de faire davantage de prévention et de sen- sibilisation à la population sur l’usage du cannabis, afin de contrer le vent de banalisation qui souffle à travers le Québec. Le train est parti, et nous n’avons plus le choix d’embarquer. 7 FÉVRIER – Marie-Ève Goyer, M.D. Fentanyl, naloxone à emporter et autres nouveautés sur les opioïdes 7 MARS – Louis Prévost,M.D.,syndic adjoint,Direction des enquêtes,CMQ Le médecin, la télémédecine, le courriel et les médias sociaux : un ménage à quatre réussi ! 4 AVRIL – À confirmer 2 MAI – À confirmer 6 JUIN – Jamie Dow, M.D., conseiller médical en sécurité routière, SAAQ L’évaluation médicale de l’aptitude à conduire un véhicule automobile TÉLÉCONFÉRENCES DE L’AMPQ EN FORMAT WEBINAIRES – HIVER 2018 12 h – 13 h Changement de dates : 1er mercredi du mois Vous souhaitez proposer des conférenciers ou des sujets pour les téléconférences ? Communiquez avec Caroline Piecha au 514 350-5108 ou par courriel cpiecha@fmsq.org. Disponible en différé sur la plateforme Méduse de la FMSQ. La tenue de cette activité a été rendue possible grâce à une subvention à visée éducative de HLS Therapeutics et Janssen Inc.
- 13. SUITE » CONTINUED » 13 LEJOURNALDEL’AMPQ•DÉCEMBRE2017 13 AQPPEP, the Association québécoise des programmes pour premiers épisodes psychotiques (Québec asso- ciation of programs for first-episode psychosis) groups together clinical professionals who work with victims of a first-episode psychosis (FEP). Its mandate includes developing public awareness to lessen the stigmatization of persons affected by a FEP, improving the identification process of such persons, referring them to appropriate services, as well as building awareness for FEP-related issues among health network administrators, political authorities, and the public. In the context of the legalization of cannabis, planned for July 2018, we wish to express our concerns about the risks of its use by several groups, and to highlight the importance of informing the public on the risks of cannabis on mental health, particularly when its use starts at adolescence or early adulthood. The risk of psychosis is evaluated at 3% in the general popu- lation, and this estimation can climb from 10 to 50% in the event of first-degree family history. The link between the use of cannabis and the increase of the risk of psychotic disor- der is undeniable 1-2 . Where the risk of psychosis increases to 40% for those who have used cannabis 3 , it is doubled for daily users (even more with high THC concentration), and even 3.9 times more among heavy users 4 . A THC concentration of 10% or more is often used as a standard of high concentration—no doubt about it. Furthermore, a FEP among cannabis users tends to happen on the aver- age 2.7 years earlier 5 , a fact, which has an impact on its prognosis. The use of cannabis before the age of 16 is specifically linked to a greater probability of psychotic symptoms 10 years later 6 , maybe even more among young persons with genetic risk factors 7 . However, the data on the interaction between a gene and the risk of psychosis remains inconsistent, and needs to be replicated 8 . Besides the risks of psychosis, the use of cannabis causes (particularly when regular use started at adolescence) cog- nitive disorders, which can last for the long-term 9 , with an influence on school results 10 . We know that the 9% risk of dependency among those who experiment with cannabis increases to 16% for those who started at adolescence 11 , the average period of initiation to the drug according to the 2012 Canadian Alcohol and Drug Use Monitoring Survey (CADUMS). This is a real concern. That’s why the AQPPEP joined both AMPQ’s and FMSQ’s positions, in line with the conclusions of Coffee and Patton 10 stating that if cannabis was ever to be legalized, the fact that the brain continues to grow into the twenties should be an argument to limit its sale to those under 21. L’AQPPEP, Association québécoise des programmes pour premiers épisodes psychotiques, est un organisme qui regroupe des professionnels de cliniques œuvrant auprès de personnes victimes d’un premier épisode psychotique (PEP). Elle a pour mandat notamment de participer à la sensibilisation du public pour diminuer la stigmatisation des personnes souffrant d’un PEP, d’améliorer l’identifica- tion et la référence de ces personnes vers des services appropriés, ainsi que de sensibiliser les administrateurs du réseau de la santé, les autorités politiques et la population à l’importance des enjeux reliés aux PEP. Dans le contexte de la légalisation du cannabis prévue pour juillet 2018, nous exprimons nos préoccupations face aux risques d’une telle consommation pour plusieurs per- sonnes. Nous voulons souligner l’importance d’informer la population sur les risques de la consommation de canna- bis pour la santé mentale, surtout lorsque celle-ci débute à l’adolescence ou au début de l’âge adulte. Le risque de psychose est évalué à 3 % dans la popula- tion générale, et cette estimation peut augmenter de 10 à 50 % en cas d’antécédents familiaux du premier degré. Le lien entre la consommation de cannabis et l’augmen- tation du risque de trouble psychotique est indéniable 1-2 . Alors que le risque de psychose augmente de 40 % chez les personnes ayant déjà consommé du cannabis 3 , il est doublé chez les consommateurs quotidiens (surtout si la concentration en THC est forte) et même 3,9 fois plus chez les gros consommateurs 4 . Une concentration de THC de 10 % et plus est souvent utilisée pour désigner une concentration élevée – ce qui n’est pas sans équi- voque. De plus, le PEP chez les consommateurs de can- nabis tend à survenir en moyenne 2,7 ans plus tôt 5 , ce qui a un impact sur son pronostic. L’utilisation de cannabis avant l’âge de 16 ans est particu- lièrement associée à une plus grande probabilité de pré- senter des symptômes psychotiques 10 ans plus tard 6 , peut-être même davantage chez des jeunes présentant des facteurs de risque génétique 7 . Toutefois, les données sur l’interaction entre un gène particulier et le risque de psychose demeurent inconsistantes et ont besoin d’être répliquées 8 . En plus des risques de psychose, la consommation de cannabis cause, notamment lorsque l’usage régulier a débuté à l’adolescence, des troubles cognitifs pouvant persister à long terme 9 , ce qui influence négativement le taux de succès scolaires 10 . Sachant le risque de dépen- dance de 9 % chez les personnes qui expérimentent le cannabis, taux qui augmente à 16 % si le cannabis est débuté à l’adolescence 11 , l’âge moyen de 16 ans d’initia- tion à la drogue chez les jeunes selon l’Enquête de sur- veillance canadienne de la consommation d’alcool et de Sophie L’Heureux, M.D. Amal Abdel-Baki, M.D. Clairélaine Ouellet- Plamondon, M.D. David Olivier, M.D. Marie Villeneuve, M.D. Aldanie Rho, M.D. FUMER UN PEU, BEAUCOUP, À LA FOLIE OU PAS DU TOUT SMOKE A LITTLE, MORE, A LOT, OR NOT AT ALL
- 14. 14 SUITE » CONTINUED » LEJOURNALDEL’AMPQ•DÉCEMBRE2017 14 Even though some psychoses are called “toxic” because they’re directly induced by the drug, some follow-up studies of persons diagnosed with a cannabis-induced toxic psych- osis 12-13-14-15 have shown that up to 50% of them have developed a schizophrenia spectrum disorder, a propor- tion, which climbed to 77% when we include all primary psychotic disorders (such as Type 1 bipolar disorders), even in the absence of any genetic history. This data sug- gests that psychiatrists tend to over-evaluate the etiological contribution of cannabis in the presentation of psychotic symptoms, when often the situation really is a primary psychosis triggered or aggravated by using cannabis. Psychiatrists who work in various gateway positions (emer- gency, evaluation-liaison modules, point of entry into the mental health system), thus have a crucial role to play in the detection of psychotic disorders to avoid repeated diagnoses of toxic psychosis, which delay the access to appropriate intensive readaptation services, even more so when the increased length of a non-treated psychosis has a direct impact on the prognosis 16 . It is therefore essential that frontline psychiatrists adopt a psycho educational approach, for the young person and his family, focused on cannabis as a trigger of severe and lasting psychotic dis- orders, and refer these young persons to a team who can refine the diagnosis, and offer the appropriate follow-up. It is equally important to adopt a motivational approach by avoiding guilt-generating comments, considering that these have little effect on the use of cannabis, and a nega- tive impact both on the therapeutic alliance, and the desire to engage in care. Last year, Québec’s MSSS announced that it would add about 15 FEP clinics throughout the province, and more specifically in regions where mental health services are lacking. However, the 19 early-inter- vention clinics, established through the involvement of clinicians, still lack resources—a challenge to face in order to give appropriate care to young Quebecers developing a FEP. In the context of the legalization of cannabis, other investments must be made to educate the public on the potential health impact of cannabis. Forty-five percent of young persons with a FEP are also affected by a cannabis use disorder 17 . For those who develop schizophrenia, the use of cannabis is linked to an increase in symptoms and relapse 18-19 . On the other hand, the cessation of use improves the prognosis after a FEP, both for psychotic symptoms and for function 20-21-22 . Indeed, close to a third of persons with a FEP stop con- suming substances in the first year after their admission to a FEP Program; among those who present a cannabis use disorder at admission, 36.6% are in remission after a year, and 47.5% after two years 17 . Among those who stopped consuming, the evolution is similar to those who have never had a cannabis use disorder, while those who keep abusing cannabis have a bad prognosis, and their symptoms keep deteriorating (psychosis and depression) as well as their ability to function (job, school, housing autonomy), despite the follow-up between the first and the second year, which suggests a pernicious effect of this substance. Moreover, those young persons with a cannabis use disorder are more often hospitalized, and consult emergencies, and generate important costs for the health system. 19 We can only hope to improve the condition of young persons through awareness campaigns targeted for and adapted to them, early detection, integrated treatment of both disorders, and increased research in the domain. drogue (2012) est jugé préoccupant. L’AQPPEP a donc joint sa voix à la position de l’AMPQ et la FMSQ, appuyée sur les écrits de Coffee et Patton 10 qui concluaient que si le cannabis devait être légalisé, le constat selon lequel le développement du cerveau se poursuit jusque dans la vingtaine devrait être un argument important pour rendre illégale sa vente aux gens de moins de 21 ans. Quoique certaines psychoses soient dites « toxiques » car directement induites par la drogue, des études de suivi de personnes diagnostiquées avec psychose toxique au cannabis 12-13-14-15 ont montré que jusqu’à 50 % ont déve- loppé un trouble du spectre de la schizophrénie, propor- tion qui monte à 77 % lorsqu’on inclut tous les troubles psychotiques primaires (dont les maladies bipolaires de type I), et ce même en l’absence d’antécédent génétique. Ces données suggèrent que les psychiatres ont tendance à surestimer la contribution étiologique du cannabis dans la présentation des symptômes psychotiques alors qu’il s’agit souvent d’une psychose primaire déclenchée ou exacerbée par la consommation de cannabis. Les psychiatres qui œuvrent aux différentes portes d’en- trée (urgence, modules d’évaluation-liaison, guichets d’accès en santé mentale) ont donc un rôle primordial à jouer dans la détection de ces troubles psychotiques afin d’éviter des diagnostics répétés de psychose toxique retardant l’accès aux services de réadaptation intensive appropriés, d’autant plus qu’une durée de psychose non traitée plus longue a un impact direct sur le pronostic 16 . Il est donc essentiel pour les psychiatres en première ligne d’adopter une approche psychoéducative, tant pour le jeune que pour ses proches, sur la contribution du canna- bis au déclenchement de troubles psychotiques graves et persistants, et de référer ces jeunes à une équipe ayant la capacité de préciser le diagnostic et d’offrir le suivi requis. Il importe également d’adopter une approche motivation- nelle en évitant des propos culpabilisants, ceux-ci ayant souvent peu d’impact sur la consommation alors qu’ils ont un impact négatif sur l’alliance thérapeutique et l’engage- ment aux soins. Dans la dernière année, le MSSS a annon- cé l’ajout d’une quinzaine de cliniques pour PEP à travers la province, notamment dans les régions où les ressources en santé mentale étaient déficientes. Toutefois, la mise à niveau des 19 cliniques d’intervention précoce déjà mises en place suite à l’initiative de cliniciens, manquent de res- sources – un autre défi à relever pour permettre aux jeunes Québécois développant un PEP de recevoir les soins ap- propriés. Dans le contexte de la légalisation du cannabis, d’autres investissements devront permettre l’éducation du grand public sur l’impact potentiel du cannabis sur la santé. Quarante-cinq pour cent des jeunes souffrant d’un PEP sont atteints d’un trouble de l’usage du cannabis 17 . Pour les personnes qui développent la schizophrénie, la consommation de cannabis est associée à davantage de symptômes et de rechutes 18-19 . À l’inverse, l’arrêt de la consommation améliore le pronostic après un PEP, tant au niveau des symptômes de psychose que du fonction- nement 20-21-22 . En effet, près du tiers des personnes pré- sentant un PEP cessent l’usage de substances dans la première année suivant l’admission à un programme pour PEP ; parmi ceux présentant un trouble de l’usage de can- nabis à l’admission, 36,6 % sont en rémission après une année et 47,5 % après 2 ans 17 . Chez ceux qui ont cessé la consommation, l’évolution est similaire à ceux n’ayant ja- mais eu un trouble de l’usage de cannabis, alors que ceux qui continuent à consommer abusivement du cannabis ont
- 15. 15 SUITE » CONTINUED » LEJOURNALDEL’AMPQ•DÉCEMBRE2017 15 IMAGE 1: Impact of substance abuse at various phases of developing a FEP Solid evidence is readily available to feed and support discussions on the subject with our patients and their family as well as with public instances. The objective, however, is not to use this data to demonize cannabis— that would produce to reverse effect—but to enrich the dialogue. The decision to legalize cannabis potentially involves an adverse impact on the health of its users. That’s why the government has the obligation to make the public—young people specifically—aware of the effects of cannabis and its health risks. The objective here is to shed light on the use of cannabis, and to prevent legalization from being perceived by young people as a green light to a harm- less practice. Psychiatrists must contribute to the debate by informing the public and the decision makers on the risks linked to the use of cannabis by young people. They must also make decision makers aware of the importance of limiting the negative impacts of legalization through specific measures. Indeed, the government must rapidly raise awareness and educate the public, most specifically young persons and those around them, and ensure that medical care is made more accessible to those who be- come addicted or develop a FEP. REFERENCES 1. Arseneault L, Cannon M, Witton J, Murray RM (2004). Causal association between cannabis and psychosis: examination of the evidence. Br J Psychiatry, 184:110-7. 2. Van Os J, Bak M, Hanssen M, Bijl RV, de Graaf R, Verdoux H (2002). Cannabis use and psychosis: a longitudinal population-based study. Am J Epidemiol. 156(4):319-27. 3. Moore TH, Zammit S, Lingford-Hughes A, Barnes TR, Jones PB, Burke M, Lewis G (2007). Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet. 370(9584):319-28. 4. Marconi A, Di Forti M, Lewis CM, Murray RM, Vassos E (2016). Meta- analysis of the Association Between the Level of Cannabis Use and Risk of Psychosis. Schizophr Bull. 42(5):1262-9. 5. Large M, Mullin K, Gupta P, Harris A, & Nielssen O (2014). Systematic meta-analysis of outcomes associated with psychosis and co-morbid substance use. Aust N Z J Psychiatry, 48:418–432. 6. Arseneault L, Cannon M, Poulton R, Murray R, Moffitt TE (2002). Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study. BMJ, 325(7374):1212–1213. 7. Caspi A, Moffitt TE, Cannon M, McClay J, Murray R, Harrington H, Taylor A, Arseneault L, Williams B, Braithwaite A, Poulton R, Craig IW (2005). Moderation of the effect of adolescent-onset cannabis use on adult psychosis by a functional polymorphism in the catechol-O- methyltransferase gene: longitudinal evidence of a gene X environment interaction. Biol Psychiatry, 57(10):1117-27. 8. Modinos G, Iyegbe C, Prata D, Rivera M, Kempton MJ, Valmaggia LR, Sham PC, van Os J, McGuire P. (2013). Molecular genetic gene- environment studies using candidate genes in schizophrenia: a systematic review. Schizophr Res. 150(2-3):356-65. 9. Crean RD, Crane NA, Mason BJ (2011) An evidence based review of acute and long-term effects of cannabis use on executive cognitive functions. J Addic Med, 5(1):1-8. 10. Coffey C, Patton GC (2016). Cannabis use in adolescence and young adulthood: A review of findings from the Victorian Adolescent Health Cohort study. Can J Psychiatry, 61(6):318-27 un mauvais pronostic, et continuent à se détériorer au niveau symptomatique (psychotique et dépressif) et fonc- tionnel (emploi, études, autonomie en hébergement), et ce malgré le suivi entre la 1re et la 2e année, suggérant un effet délétère de cette substance. De plus, ces jeunes avec trouble de l’usage de cannabis sont plus souvent hospita- lisés et consultent plus à l’urgence, engendrant ainsi des coûts importants pour le système de santé 19 . On peut espérer qu’avec des campagnes de sensibilisa- tion ciblées et adaptées aux jeunes, une détection pré- coce, un traitement intégré des deux troubles et plus de recherches dans le domaine, on réussira à améliorer l’évo- lution de ces jeunes. IMAGE 1 : Impact de la toxicomanie à différentes phases du développement d’un PEP Les données probantes disponibles peuvent alimenter les discussions avec nos patients et leurs proches ainsi qu’avec les instances publiques. L’objectif n’est toutefois pas de les utiliser pour démoniser le cannabis, ce qui au- rait probablement l’effet inverse, mais plutôt pour appro- fondir le dialogue. Dans le contexte de la légalisation du cannabis, le gou- vernement a le devoir de s’assurer qu’une sensibilisation soit faite auprès du grand public et plus spécifiquement auprès des jeunes, quant aux effets du cannabis et à ses risques pour la santé. L’objectif est d’éclairer la décision de consommer et d’éviter que le message compris par les jeunes soit que légalisation signifie absence de dan- ger. Les psychiatres doivent contribuer au débat en infor- mant la population et les décideurs sur les risques liés à la consommation de cannabis chez les jeunes, tout en faisant valoir aux décideurs l’importance de prendre les mesures nécessaires pour limiter les impacts négatifs de la légalisation. En effet, le gouvernement doit s’assurer d’entreprendre rapidement la sensibilisation et l’éduca- tion du public, notamment des jeunes eux-mêmes et des personnes qui les côtoient, mais également s’assurer de rendre plus accessibles les soins médicaux aux personnes qui deviendraient dépendantes de cette substance ou qui développeraient un PEP. RÉFÉRENCES 1. Arseneault L, Cannon M, Witton J, Murray RM (2004). Causal association between cannabis and psychosis: examination of the evidence. Br J Psychiatry, 184:110-7. 2. Van Os J, Bak M, Hanssen M, Bijl RV, de Graaf R, Verdoux H (2002). Cannabis use and psychosis: a longitudinal population-based study. Am J Epidemiol. 156(4):319-27. 3. Moore TH, Zammit S, Lingford-Hughes A, Barnes TR, Jones PB, Burke M, Lewis G (2007). Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet. 370(9584):319-28. 4. Marconi A, Di Forti M, Lewis CM, Murray RM, Vassos E (2016). Meta- analysis of the Association Between the Level of Cannabis Use and Risk of Psychosis. Schizophr Bull. 42(5):1262-9. 5. Large M, Mullin K, Gupta P, Harris A, & Nielssen O (2014). Systematic meta-analysis of outcomes associated with psychosis and co-morbid substance use. Aust N Z J Psychiatry, 48:418–432. Facteurs génétiques psychose chez un membre de la famille Facteurs de l’environnement • Toxicomanie • Facteurs de stress de la vie Facteurs biologiques Ex. Complications grossesse / accouchement PEP Facteurs de l’environnement • Toxicomanie • Facteurs de stress de la vie État mental à à risque de psychose symptômes à bas bruits de psychose Facteurs influents sur le pronostic : • Observance Rx • Toxicomanie • Facteurs de stress Genetic factors Psychosis in a family member Environmental factors • Substance abuse • Life stress factors Biological factors i.e.:complications during pregnancy/ childbirth FEP Environmental factors • Substance abuse • Life stress factors Mental state as risk of psychosis Low profile symptoms of psychosis Factors influencing the prognosis: • Rx compliance • Sustance abuse • Stress factors
- 16. 16 LEJOURNALDEL’AMPQ•DÉCEMBRE2017 16 11. Volkow, Nora D., M.D., Ruben D. Baler, Ph.D., Wilson M. Compton, M.D., and Susan R.B. Weiss, Ph.D. Adverse Health Effects of Marijuana Use, N Engl J Med 2014; 370:2219-2227June 5, 2014DOI: 10.1056/ NEJMra1402309 12. Arendt M, Rosenberg R, Foldager L, Perto G, Munk-Jørgensen P (2005). Cannabis-induced psychosis and subsequent schizophrenia- spectrum disorders: follow-up study of 535 incident cases. Br J Psychiatry, 187, 510-515. 13. Arendt M, Mortensen PB, Rosenberg R, Pedersen CB, Waltoft BL (2008). Familial Predisposition for Psychiatric Disorder - Comparison of Subjects Treated for Cannabis-Induced Psychosis and Schizophrenia. Arch Gen Psychiatry, 65(11):1269-1274. 14. Alderson HL, Semple DM, Blayney C, Queirazza F, Chekuri V, Lawrie SM. (2017) Risk of transition to schizophrenia following first admission with substance-induced psychotic disorder: a population-based longitudinal cohort study. Psychol Med. 47(14):2548-2555. 15. Niemi-Pynttäri JA, Sund R, Putkonen H, Vorma H, Wahlbeck K, Pirkola SP (2013) Substance-induced psychoses converting into schizophrenia: a register-based study of 18,478 Finnish inpatient cases. J Clin Psychiatry. 74(1): e94-9. 16. Penttilä M, Jääskeläinen E, Hirvonen N, Isohanni M, Miettunen J (2014). Duration of untreated psychosis as predictor of long-term outcome in schizophrenia: systematic review and meta-analysis. Br J Psychiatry. 205(2):88-94. 17. Abdel-Baki A, Ouellet-Plamondon C, Salvat E, Grar K, Potvin S. (2017). Symptomatic and functional outcomes of substance use disorder persistence 2 years after admission to a first-episode psychosis program. Psychiatry Research, 247, 113-119. 18. Schoeler T, Monk A, Sami MB, Klamerus E, Foglia E, Brown R, Camuri G, Altamura AC, Murray R, & Bhattacharyya S (2016). Continued versus discontinued cannabis use in patients with psychosis: a systematic review and meta-analysis. Lancet Psychiatry, 3:215–225. 19. Ouellet-Plamondon C, Abdel-Baki A, Salvat E, Potvin S (2017). Specific impact of stimulant, alcohol and cannabis use disorders on first-episode psychosis: 2-year functional and symptomatic outcomes. Psychol Med. 47(14):2461-2471. 20. Mullin K, Gupta P, Compton MT, Large M (2012). Does giving up substance use work for patients with psychosis? A systematic meta- analysis. Aust N Z J Psychiatry, 46(9):826-39. 21. Turkington A, Mulholland CC, Rushe TM, Anderson R, McCaul R, Barrett SL, Barr RS, & Cooper SJ (2009). Impact of persistent substance misuse on 1-year outcome in first-episode psychosis. Br J Psychiatry, 195:242–248. 22. Harrison, I, Joyce EM, Mutsatsa SH, Hutton SB, Huddy V, Kapasi M, & Barnes TRE (2008). Naturalistic follow-up of co-morbid substance use in schizophrenia: the West London first-episode study. Psychological Medicine, 38:79–88. ADDITIONAL REFERENCES Bourque J, Afzali MH, O’Leary-Barrett M, Conrod P (2017). Cannabis use and psychotic-like experiences trajectories during early adolescence: the coevolution and potential mediators. J Child Psychol Psychiatry. Jul 5 (epub ahead of print). Di Forti M, Sallis H, Allegri F, Trotta A, Ferraro L, Stilo SA, Marconi A, La Cascia C, Reis Marques T, Pariante C, Dazzan P, Mondelli V, Paparelli A, Kolliakou A, Prata D, Gaughran F, David AS, Morgan C, Stahl D, Khondoker M, MacCabe JH, Murray RM (2014). Daily use, especially of high-potency cannabis, drives the earlier onset of psychosis in cannabis users. Schizophr Bull, 40(6):1509-17. Linszen DH, Dingemans PM, & Lenior ME (1994). Cannabis abuse and the course of recent-onset schizophrenic disorders. Arch Gen Psychiatry, 51:273–279. 6. Arseneault L, Cannon M, Poulton R, Murray R, Moffitt TE (2002). Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study. BMJ, 325(7374):1212–1213. 7. Caspi A, Moffitt TE, Cannon M, McClay J, Murray R, Harrington H, Taylor A, Arseneault L, Williams B, Braithwaite A, Poulton R, Craig IW (2005). Moderation of the effect of adolescent-onset cannabis use on adult psychosis by a functional polymorphism in the catechol-O- methyltransferase gene: longitudinal evidence of a gene X environment interaction. Biol Psychiatry, 57(10):1117-27. 8. Modinos G, Iyegbe C, Prata D, Rivera M, Kempton MJ, Valmaggia LR, Sham PC, van Os J, McGuire P. (2013). Molecular genetic gene- environment studies using candidate genes in schizophrenia: a systematic review. Schizophr Res. 150(2-3):356-65. 9. Crean RD, Crane NA, Mason BJ (2011) An evidence based review of acute and long-term effects of cannabis use on executive cognitive functions. J Addic Med, 5(1):1-8. 10. Coffey C, Patton GC (2016). Cannabis use in adolescence and young adulthood: A review of findings from the Victorian Adolescent Health Cohort study. Can J Psychiatry, 61(6):318-27 11. Volkow, Nora D., M.D., Ruben D. Baler, Ph.D., Wilson M. Compton, M.D., and Susan R.B. Weiss, Ph.D. Adverse Health Effects of Marijuana Use, N Engl J Med 2014; 370:2219-2227June 5, 2014DOI: 10.1056/ NEJMra1402309 12. Arendt M, Rosenberg R, Foldager L, Perto G, Munk-Jørgensen P (2005). Cannabis-induced psychosis and subsequent schizophrenia- spectrum disorders: follow-up study of 535 incident cases. Br J Psychiatry, 187, 510-515. 13. Arendt M, Mortensen PB, Rosenberg R, Pedersen CB, Waltoft BL (2008). Familial Predisposition for Psychiatric Disorder - Comparison of Subjects Treated for Cannabis-Induced Psychosis and Schizophrenia. Arch Gen Psychiatry, 65(11):1269-1274. 14. Alderson HL, Semple DM, Blayney C, Queirazza F, Chekuri V, Lawrie SM. (2017) Risk of transition to schizophrenia following first admission with substance-induced psychotic disorder: a population-based longitudinal cohort study. Psychol Med. 47(14):2548-2555. 15. Niemi-Pynttäri JA, Sund R, Putkonen H, Vorma H, Wahlbeck K, Pirkola SP (2013) Substance-induced psychoses converting into schizophrenia: a register-based study of 18,478 Finnish inpatient cases. J Clin Psychiatry. 74(1): e94-9. 16. Penttilä M, Jääskeläinen E, Hirvonen N, Isohanni M, Miettunen J (2014). Duration of untreated psychosis as predictor of long-term outcome in schizophrenia: systematic review and meta-analysis. Br J Psychiatry. 205(2):88-94. 17. Abdel-Baki A, Ouellet-Plamondon C, Salvat E, Grar K, Potvin S. (2017). Symptomatic and functional outcomes of substance use disorder persistence 2 years after admission to a first-episode psychosis program. Psychiatry Research, 247, 113-119. 18. Schoeler T, Monk A, Sami MB, Klamerus E, Foglia E, Brown R, Camuri G, Altamura AC, Murray R, & Bhattacharyya S (2016). Continued versus discontinued cannabis use in patients with psychosis: a systematic review and meta-analysis. Lancet Psychiatry, 3:215–225. 19. Ouellet-Plamondon C, Abdel-Baki A, Salvat E, Potvin S (2017). Specific impact of stimulant, alcohol and cannabis use disorders on first-episode psychosis: 2-year functional and symptomatic outcomes. Psychol Med. 47(14):2461-2471. 20. Mullin K, Gupta P, Compton MT, Large M (2012). Does giving up substance use work for patients with psychosis? A systematic meta- analysis. Aust N Z J Psychiatry, 46(9):826-39. 21. Turkington A, Mulholland CC, Rushe TM, Anderson R, McCaul R, Barrett SL, Barr RS, & Cooper SJ (2009). Impact of persistent substance misuse on 1-year outcome in first-episode psychosis. Br J Psychiatry, 195:242–248. 22. Harrison, I, Joyce EM, Mutsatsa SH, Hutton SB, Huddy V, Kapasi M, & Barnes TRE (2008). Naturalistic follow-up of co-morbid substance use in schizophrenia: the West London first-episode study. Psychological Medicine, 38:79–88. RÉFÉRENCES ADDITIONNELLES Bourque J, Afzali MH, O’Leary-Barrett M, Conrod P (2017). Cannabis use and psychotic-like experiences trajectories during early adolescence: the coevolution and potential mediators. J Child Psychol Psychiatry. Jul 5 (epub ahead of print). Di Forti M, Sallis H, Allegri F, Trotta A, Ferraro L, Stilo SA, Marconi A, La Cascia C, Reis Marques T, Pariante C, Dazzan P, Mondelli V, Paparelli A, Kolliakou A, Prata D, Gaughran F, David AS, Morgan C, Stahl D, Khondoker M, MacCabe JH, Murray RM (2014). Daily use, especially of high-potency cannabis, drives the earlier onset of psychosis in cannabis users. Schizophr Bull, 40(6):1509-17. Linszen DH, Dingemans PM, & Lenior ME (1994). Cannabis abuse and the course of recent-onset schizophrenic disorders. Arch Gen Psychiatry, 51:273–279.