Leading the Charge to Change the Obesity Narrative: Supporting Primary Care to Improve Weight Management Discussions, Diagnosis, and Decisions
•
0 likes•4 views

Co-Chairs, Jaime Almandoz, MD, MBA, FTOS, and Angela Fitch, MD, FACP, FOMA, prepared useful Practice Aids pertaining to obesity for this CME activity titled “Leading the Charge to Change the Obesity Narrative: Supporting Primary Care to Improve Weight Management Discussions, Diagnosis, and Decisions.” For the full presentation, downloadable Practice Aids, and complete CME information, and to apply for credit, please visit us at https://bit.ly/42vnSPs. CME credit will be available until September 17, 2024.

Recommended
More Related Content
Similar to Leading the Charge to Change the Obesity Narrative: Supporting Primary Care to Improve Weight Management Discussions, Diagnosis, and Decisions
Similar to Leading the Charge to Change the Obesity Narrative: Supporting Primary Care to Improve Weight Management Discussions, Diagnosis, and Decisions (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Leading the Charge to Change the Obesity Narrative: Supporting Primary Care to Improve Weight Management Discussions, Diagnosis, and Decisions
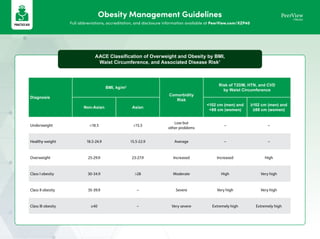
- 1. Obesity Management Guidelines Full abbreviations, accreditation, and disclosure information available at PeerView.com/XZP40 Obesity AACE Classification of Overweight and Obesity by BMI, Waist Circumference, and Associated Disease Risk1 Diagnosis BMI, kg/m2 Comorbidity Risk Risk of T2DM, HTN, and CVD by Waist Circumference Non-Asian Asian <102 cm (men) and <88 cm (women) ≥102 cm (men) and ≥88 cm (women) Underweight <18.5 <15.5 Low but other problems – – Healthy weight 18.5-24.9 15.5-22.9 Average – – Overweight 25-29.9 23-27.9 Increased Increased High Class I obesity 30-34.9 >28 Moderate High Very high Class II obesity 35-39.9 – Severe Very high Very high Class III obesity ≥40 – Very severe Extremely high Extremely high
- 2. Obesity Management Guidelines Full abbreviations, accreditation, and disclosure information available at PeerView.com/XZP40 Obesity a Tirzepatide is not currently approved for obesity; it is currently indicated for glucose-lowering in T2DM. b BMI ≥25 kg/m2 in Asian individuals. c BMI ≥27.5 kg/m2 in Asian individuals. d Use phentermine/topiramate with caution. e Monitor all patients for depression and suicidal thoughts, discontinue if symptoms develop. f Liraglutide and semaglutide are associated with reduced MACE in PwT2D; tirzepatide does not increase MACE risk in PwT2D. CVOTs in PwO are ongoing. 1. https://pro.aace.com/files/obesity/toolkit/classification_of_obesity_and_risks.pdf. 2. https://www.accessdata.fda.gov/scripts/cder/daf/. 3. Chakhtoura M et al. eClinicalMedicine. 2023;58:101882. 4. NIH. Am J Clin Nutr. 1992;55(2 Suppl):615S-619S. 5. Eisenberg D et al. Obes Surg. 2023;33:3-14. 6. Guan R et al. Front Pharmacol. 2022;13:998816. 7. Gastaldelli A et al. Diabetologia. 2021;64(suppl 1):S219-S220. Suggested Obesity Treatment Algorithm2-6,a BMI ≥30 or ≥27 kg/m2 with ≥1 comorbidity BMI ≥30 kg/m2b with T2DM or BMI ≥30 kg/m2b without substantial or durable weight loss or comorbidity improvement using nonsurgical methods or BMI ≥35 kg/m2 with ≥1 adverse health consequence because of obesity or BMI ≥40 kg/m2c CVD and T2DMe Comorbidities Depressiond,e History of MTCf No NAFLD Yes Obstructive sleep apnea Opioid use or history of seizure Uncontrolled HTN Lifestyle modification Cessation of weight-inducing medications Bariatric surgery Liraglutide Orlistat Semaglutide Tirzepatidea All medications Liraglutide Naltrexone/bupropion Orlistat Phentermine/topiramate Semaglutide Tirzepatidea Naltrexone/bupropion Orlistat Phentermine/ topiramate Liraglutide Orlistat Semaglutide Tirzepatide7,a Liraglutide Naltrexone/bupropion Orlistat Phentermine/topiramate Semaglutide Tirzepatidea Liraglutide Orlistat Phentermine/ topiramate Semaglutide Liraglutide Orlistat Semaglutide Tirzepatidea Treatment options are listed in alphabetical order, not by preference of use
- 3. Obesity Guidance on Conducting a Weight Management Visit Full abbreviations, accreditation, and disclosure information available at PeerView.com/XZP40 Weight Loss Conversation Guide Would it be okay if we discussed your weight and your health today? I would be happy to set up an appointment with you to follow up when you are ready. May I share my concerns about your health? Would you like help losing weight? Reason for Losing Weight How Much Weight Loss Is Needed Suggestions for Losing It • Reduce blood glucose and triglycerides 3% Lifestyle modification (2%-5% loss) • Increase HDL-C • Reduce BP, liver fat (NAFLD), and/or urinary stress incontinence • Improved sexual function and/or QOL 5% Lifestyle modification (2%-5%) Prescriptive nutritional intervention (5%-10%) • Reduce NASH activity and/or sleep apnea 10% Prescriptive nutritional intervention (5%-10%) Pharmacotherapy (10%-25%) • Reduce risk of heart attack or stroke • Reverse T2DM • Reduce the risk of death 15% Pharmacotherapy (10%-25%) Endoscopic procedures (10%-20%) Yes Yes No No Yes
- 4. Recommendations for Creating Patient-Centered Obesity Treatment Plans Diagnose Diagnose obesity by class; class I (BMI 30-34.9), class II (BMI 35- 39.9), and class III (BMI ≥40) Consider stage of disease by severity of comorbidities Prescribe a nutritional plan • Track food intake (eg, LoseIt, MyFitnessPal) • Meal replacement plan like LookAHEAD or VLCD • Prescriptive nutritional intervention • Planned portions of plants and protein Determine an activity goal A minimum of 150 min (2 h and 30 min) per week of moderate intensity aerobic physical activity or 75 min (1 h and 15 min) of vigorous intensity physical activity is recommended1,2 Prescribe medication if BMI ≥27 with major medical condition or ≥30 alone Talk to patient about using medication to be 2-4 times more likely to lose weight successfully and maintain loss Prescribe surgery when indicated Evaluate surgery anatomy if past history of surgery—upper GI and/or EGD as indicated Arrange follow up 1-3 mo—the more accountability the better Consider remote monitoring or chronic care management for more accountability Prescribe Determine Evaluate Prescribe Arrange Consider Obesity Guidance on Conducting a Weight Management Visit Full abbreviations, accreditation, and disclosure information available at PeerView.com/XZP40
- 5. 1. https://www.cdc.gov/physicalactivity/basics/adults/index.htm. 2. https://obesitymedicine.org/physical-fitness-and-physical-activity/. Communication Tools: Resources for Talking With Patients About Obesity OMA: Motivational Interviewing Guide NIDDK: Weight Management Resources for Health Professionals Obesity Action Coalition: People- First Language NIDDK: Talking With Patients About Weight Loss NIDDK: Staying Active at Any Size AACE: Keys to Successful Conversations STOP Obesity Alliance: Guide for the Management of Obesity in the Primary Care Setting AACE: Healthy Eating and Physical Activity Goal Setting Obesity Canada: 5As of Obesity Management Obesity Guidance on Conducting a Weight Management Visit Full abbreviations, accreditation, and disclosure information available at PeerView.com/XZP40
- 6. Obesity Know More About Anti-Obesity Medications Full abbreviations, accreditation, and disclosure information available at PeerView.com/XZP40 Patient-centered education and support is key in obesity management. Please use the printable resource on the following pages to support conversations about long-term anti-obesity medications with your patients. Your patients should have access to this resource at home so they can learn more about the role of anti-obesity medication in treating this chronic disease, how effective each medication may be, and which adverse reactions are commonly associated with these medications.
- 7. a Tirzepatide is not currently approved for obesity; it is currently indicated for glucose-lowering in T2DM. 1. Tak YJ, Lee SY. Curr Obes Rep. 2021;10:14-30. 2. Bays HE et al. Obesity Pillars. 2022;4:100039. 3. Matza LS et al. Patient. 2022;15:367-377. 4. Maski K et al. J Clin Sleep Med. 2021;17:1895-1945. 5. Christensen SM et al. Obesity Pillars. 2022;4:100041. 6. Redmond IP et al. Curr Obes Rep. 2021;10:81-99. 7. Jastreboff AM et al. N Engl J Med. 2022;387:205-216. Effectively Managing Your Obesity: Aligning Treatment With the Right Medication1-7 Ways in Which Treatment Can Help Recommended Medications to Consider Nutrition • Prevents fat absorption from food1 • Orlistat • Slows down digestion1 • Liraglutide and semaglutide Physical activity • Increases one’s desire to be active with weight loss2,3 • Tirzepatidea Behavior • Reduces appetite1,3 • Phentermine/topiramate, naltrexone/bupropion, liraglutide, semaglutide, and tirzepatidea • Reduces cravings and/or binge eating1,3 • Naltrexone/bupropion, phentermine/topiramate, liraglutide, semaglutide, and tirzepatidea • Increases sense of fullness1 • Liraglutide, semaglutide, and hydrogel • Improves sleep3,4 • Liraglutide and tirzepatidea Medication • May prevent weight gain caused by other medications, including but not limited to medications for depression, schizophrenia, bipolar disorder, and insulin5 • See the next page for more information Bariatric procedures • Prevent weight regain after bariatric surgery6 • Partly reverse weight gain after surgery6 • Liraglutide, semaglutide, tirzepatide,a orlistat, and phentermine/topiramate Pairing weight loss medication with behavioral changes like learning to eat more slowly, noticing when you feel full, and becoming more active has a greater effect on improving your health, as research has shown (see next page).
- 8. a Greater weight loss is likely if combined with intensive behavioral therapy. b Tirzepatide is not currently approved for obesity; it is currently indicated for glucose-lowering in T2DM. 1. Wilding JPH et al. N Engl J Med. 2021;384:989-1002. 2. Jebb SA et al. Lancet. 2011;378:1485-1492. 3. Maciejewski ML et al. JAMA Surg. 2016;151:1046-1055. 4. Wadden TA et al. Obesity (Silver Spring). 2011;19:110-120. 5. Wadden TA et al. Obesity (Silver Spring). 2019;27:75-86. 6. Athinarayanan SJ et al. Front Endocrinol. 2019;10:348. 7. Jastreboff AM et al. N Engl J Med. 2022;387:205-216. 8. https://www.accessdata.fda.gov/scripts/cder/daf/. 9. https://www.myplenity.com/siteassets/components/pdfs/acq_hcp_plenity-physician-ifu_march_2021.pdf. 10. Greenway FL et al. Obesity (Sliver Spring). 2019;27:205-216. What to Expect When Taking an Anti-Obesity Medication1-10 With Each Medication, How Likely Am I to Lose the Following Percentage of Weight?a What Effects Might I Experience When I Start Taking This Medication? 5% 10% 15% 20% Orlistat Taken orally, 3x/day +++ + – – • Oily spotting on underwear/clothing • Fatty/oily stool • Intestinal gas with discharge • Sudden urge to have a bowel movement • Increased number of bowel movements • Difficulty controlling bowel movements • Rectal leakage Phentermine/ topiramate ER Taken orally, 1x/day ++++ +++ ++ + • Tingling or prickling sensations • Dizziness • Change in sense of taste • Insomnia • Constipation • Dry mouth Naltrexone ER/ bupropion ER Taken orally, 2x/day +++ ++ + – • Nausea • Constipation • Headache • Vomiting • Dizziness • Insomnia • Dry mouth • Diarrhea Liraglutide 3.0 mg Once daily injection +++ ++ – – • Nausea • Diarrhea • Constipation • Vomiting • Soreness at injection site • Fever • Headache • Low blood sugar • High levels of lipase • Upper abdominal pain • Stomach flu Semaglutide 2.4 mg Once weekly injection +++++ ++++ +++ ++ • Nausea • Diarrhea • Constipation • Pain in stomach/abdomen • Low blood sugar • Stomach flu • Headache • Fatigue • Dizziness • Bloating/swelling in belly • Belching • Flatulence • Gastroesophageal reflux disease Tirzepatideb Once weekly injection +++++ +++++ ++++ ++++ • Nausea • Diarrhea • Decreased appetite • Vomiting • Constipation • Pain/discomfort in the stomach/abdomen Hydrogel Taken orally, 2x/day ++++ ++ – – • Diarrhea • Pain/swelling in belly • Infrequent bowel movements • Flatulence • Constipation • Nausea + = 0%-19% ++ = 20%-39% +++ = 40%-59% ++++ = 60%-79% +++++ = 80%-100%
- 9. Obesity Surveys for Primary Care Providers Full abbreviations, accreditation, and disclosure information available at PeerView.com/XZP40 Obesity Training Workshop Action Plan for Obesity Specialists Access the full suite of resources to create your own training workshop through the Education Collection: www.peerview.com/ObesityTrainingCenter Obesity specialists can use this page in preparation for hosting an obesity training workshop. Share pages 2-5 of this document with your primary care colleagues before and during your workshop. Step 1: Prepare Collect or develop resources to support obesity care for your practice area Invite primary care colleagues to participate in a training workshop Administer the Baseline Survey (see pages 2-3) to participants Develop an educational activity based on the needs revealed by the Baseline Survey (see pages 2-3) Step 2: Execute Include opportunities for the participants to practice the skills you taught Listen to participants’ feedback and answer their questions Ask the participants to complete the Self-Reflection Worksheet (see pages 4-5) Provide resources to participants based on their needs Step 3: Follow Up Follow up and provide ongoing support to the participants after the activity Use the feedback to refine or extend your next training workshop
- 10. Obesity Surveys for Primary Care Providers Full abbreviations, accreditation, and disclosure information available at PeerView.com/XZP40 Obesity Obesity Management Baseline Survey (page 1 of 2) Rate your comfort or level of agreement with each of the statements below. Perceived Skills 5 = strongly agree; 4 = agree; 3 = neither agree nor disagree; 2 = disagree; 1 = strongly disagree 5 4 3 2 1 I am able to assess weight status and associated risk factors I am able to address weight management and obesity issues with patients I am able to teach and motivate patients toward physical activity I am able to teach and motivate patients toward healthy eating I am able to use behavior modification techniques to make lifestyle changes in my patients I am able to deal with family issues around weight management Professional Attitudes 5 = strongly agree; 4 = agree; 3 = neither agree nor disagree; 2 = disagree; 1 = strongly disagree 5 4 3 2 1 I do not feel that obesity intervention is within my scope of practice I believe that my role is simply to raise the issue of obesity rather than intervene I do not have time to deal with the issue of obesity in my practice Obesity is too difficult an issue to tackle, therefore I do not address it in my practice I feel overwhelmed by the issue of obesity I am not confident that any obesity intervention I attempt will make a lasting difference I do not feel sufficiently educated or competent in obesity intervention strategies I do not know whom to refer patients to when obesity intervention is required I am not comfortable discussing obesity with my patients I avoid bringing up the topic of obesity as I do not want to offend or jeopardize my relationship with my patients and/or their family members As a healthcare professional, I am extremely frustrated with the low success rate in managing obesity I feel that my patients will not actually follow through on any obesity intervention, so my efforts will have little or no impact I do not feel the need to address obesity with my patients unless they look or act sick I fear that talking about obesity could do even more damage by leading my patient toward an eating disorder or other psychological problem
- 11. Obesity Surveys for Primary Care Providers Full abbreviations, accreditation, and disclosure information available at PeerView.com/XZP40 Obesity Obesity Management Baseline Survey (page 2 of 2) Rate your comfort or level of agreement with each of the statements below. Challenges 5 = strongly agree; 4 = agree; 3 = neither agree nor disagree; 2 = disagree; 1 = strongly disagree 5 4 3 2 1 Obesity intervention is not taught in my discipline’s curriculum before we enter practice There is limited professional training in this area available as continuing education Healthcare professionals in my discipline are not adequately compensated for treating obesity There is a lack of appropriate referral options (eg, dietitians or other related professionals) There is a lack of accurate patient education materials regarding obesity to distribute to our patients Healthcare professionals in my discipline need more guidance toward raising a sensitive issue such as obesity with our patients Healthcare professionals in my discipline need more guidance in motivational interviewing for behavior change related to obesity Thank you for participating!
- 12. Obesity Surveys for Primary Care Providers Full abbreviations, accreditation, and disclosure information available at PeerView.com/XZP40 Obesity Obesity Self Reflection Worksheet (page 1 of 2) What will help me remember to look beyond weight and see the whole person when meeting with patients with obesity? Do I have waiting room furniture, examination tables, wheelchairs, gowns, blood pressure cuffs, and scales that can accommodate individuals weighing >400 lb? Do I look for opportunities to discuss weight with patients, with their permission? Do I discuss weight and weight loss goals in terms of their effects on overall health?
- 13. Obesity Surveys for Primary Care Providers Full abbreviations, accreditation, and disclosure information available at PeerView.com/XZP40 Obesity Obesity Self Reflection Worksheet (page 2 of 2) Do I have realistic expectations for weight loss interventions? (eg, amount of weight loss, speed of weight loss, need for ongoing maintenance) Do I know enough about current and emerging AOMs? (eg, indications, contraindications, common adverse effects, how will they feel using this treatment, when to call the office) What other HCPs offer respectful care to patients with obesity within my practice area? (eg, obesity specialist, endocrinologist, psychiatrist, dietitian, diabetes educator, bariatric surgeon) What obesity management resources are available in my practice area? (eg, cooking/exercise classes, parks, walking trails, swimming pools, meal kit services, support groups, recreation centers)