Large Hemispheric Infarction: Exploring the Latest Clinical Advances in the Diagnosis and Treatment
•
0 likes•83 views

1. The document discusses treatment strategies for patients who have experienced a large hemispheric infarction (LHI). It provides a timeline of evidence-based therapies for LHIs including intravenous tissue plasminogen activator (tPA), endovascular thrombectomy, antithrombotic therapy, and decompressive craniectomy. 2. Emerging therapies and targets for managing cerebral edema in LHI patients are discussed, including the drugs conivaptan, fingolimod, celecoxib, and glyburide which have various mechanisms of action targeting aquaporin receptors, sphingosine-1-phosphate, cyclooxygenase-2, and SUR1/TRPM4 channels respectively

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Large Hemispheric Infarction: Exploring the Latest Clinical Advances in the Diagnosis and Treatment
Similar to Large Hemispheric Infarction: Exploring the Latest Clinical Advances in the Diagnosis and Treatment (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Large Hemispheric Infarction: Exploring the Latest Clinical Advances in the Diagnosis and Treatment
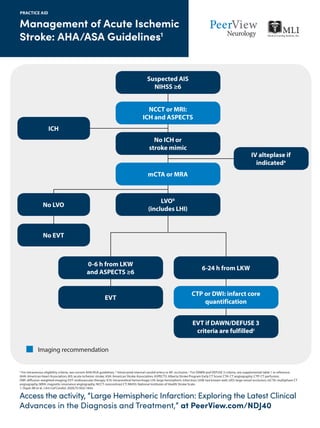
- 1. Access the activity, “Large Hemispheric Infarction: Exploring the Latest Clinical Advances in the Diagnosis and Treatment,” at PeerView.com/NDJ40 Management of Acute Ischemic Stroke: AHA/ASA Guidelines1 PRACTICE AID a For intravenous eligibility criteria, see current AHA/ASA guidelines. b Intracranial internal carotid artery or M1 occlusion. c For DAWN and DEFUSE 3 criteria, see supplemental table 1 in reference. AHA: American Heart Association; AIS: acute ischemic stroke; ASA: American Stroke Association; ASPECTS: Alberta Stroke Program Early CT Score; CTA: CT angiography; CTP: CT perfusion; DWI: diffusion-weighted imaging; EVT: endovascular therapy; ICH: intracerebral hemorrhage; LHI: large hemispheric infarction; LKW: last known well; LVO: large vessel occlusion; mCTA: multiphase CT angiography; MRA: magnetic resonance angiography; NCCT: noncontrast CT; NIHSS: National Institutes of Health Stroke Scale. 1. Ospel JM et al. J Am Coll Cardiol. 2020;75:1832-1843. Suspected AIS NIHSS ≥6 No ICH or stroke mimic IV alteplase if indicateda ICH NCCT or MRI: ICH and ASPECTS mCTA or MRA Imaging recommendation LVOb (includes LHI) No LVO No EVT 0-6 h from LKW and ASPECTS ≥6 6-24 h from LKW EVT CTP or DWI: infarct core quantification EVT if DAWN/DEFUSE 3 criteria are fulfilledc
- 2. Treatment Strategies for Patients Who Have a Large Hemispheric Infarction PRACTICE AID Access the activity, “Large Hemispheric Infarction: Exploring the Latest Clinical Advances in the Diagnosis and Treatment,” at PeerView.com/NDJ40 A Timeline of Evidence-Based Therapies for Treating Patients With an LHI Tissue plasminogen activator (tPA)1,2 • Initiate within <4.5 hours • Increases survival in patients experiencing a severe stroke Endovascular thrombectomy3-9 • Initiate within 6 hours (earlier is better) • Improves patient outcome over tPA alone Antithrombotic therapy10 • Initiate within 48 hours Decompressive craniectomy10 • Dramatically reduced mortality in patients with a malignant MCA infarction • High likelihood of permanent and severe disability Antiosmotic therapy10 • Initiate 1-4 days for cerebral edema • Mannitol and hypertonic saline are reasonable choices; avoid steroids and barbiturates
- 3. Treatment Strategies for Patients Who Have a Large Hemispheric Infarction AIS: acute ischemic stroke; AS: ankylosing spondylitis; COX-2: cyclooxygenase-2; JRA: juvenile rheumatoid arthritis; LHI: large hemispheric infarction; MCA: middle cerebral artery; MOA: mechanism of action; MS: multiple sclerosis; OA: osteoarthritis; RA: rheumatoid arthritis; S1P: sphingosine-1-phosphate; SUR1: sulfonylurea receptor 1; TRPM4: transient receptor potential cation channel subfamily M member 4. 1. Jauch EC et al. Stroke. 2013;44:870-947. 2. Demchuk AM et al. Stroke. 2005;36:2110-2115. 3. Powers WJ et al. Stroke. 2015;46:3020-3035. 4. Campbell BC et al. N Engl J Med. 2015;372:1009-1018.5. Saver JL et al. N Engl J Med. 2015;372:2285-2295. 6. Jovin TG et al. N Engl J Med. 2015;372:2296-2306. 7. Nogueira RG et al. N Engl J Med. 2018;378:11-21. 8. Goyal M et al. N Engl J Med. 2015;372:1019-1030. 9. Albers GW et al. N Engl J Med. 2018;378:708-718. 10. Torbey MT et al. Neurocrit Care. 2015;22:146-164. 11. Stokum JA et al. Annu Rev Pharmacol Toxicol. 2020;60:291-309. 12. Vaprisol (conivaptan hydrochloride). Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/021697s005lbl.pdf. 13. Gilenya (fingolimod). Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/ label/2019/022527s031lbl.pdf. 14. Celebrex (celecoxib). Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/020998s054lbl.pdf. 15. https://www.accessdata.fda.gov/scripts/opdlisting/oopd/detailedIndex.cfm?cfgridkey=20165393. PRACTICE AID Access the activity, “Large Hemispheric Infarction: Exploring the Latest Clinical Advances in the Diagnosis and Treatment,” at PeerView.com/NDJ40 Managing Cerebral Edema: Potential Targets, Emerging Therapies, and Mechanisms of Action11 • Emerging therapy: conivaptan – Currently indicated for hyponatremia12 • MOA: absorbs free water in kidneys • Emerging therapy: fingolimod – Currently indicated for relapsing MS13 • MOA: reduces vascular permeability • Emerging therapy: celecoxib – Currently indicated for OA, RA, JRA, AS, acute pain, and primary dysmenorrhea14 • MOA: reduces inflammation • Emerging therapy: glyburide – Orphan desgination for severe edema in patients who had an AIS15 • MOA: conducts monovalent cations Target: aquaporin receptor Target: S1P Target: COX-2 Target: SUR1/TRPM4