Best Practices for Recognizing & Managing Immune-Related Adverse Events in the Emergency Department: Become Aware, Stay Alert, Change Your Practice, & Keep Patients With Cancer Safe
•
1 like•36 views

Evan J. Lipson, MD, and Andrew Stolbach, MD, MPH, prepared useful practice aids pertaining to immune-related adverse effects for this CME/MOC/CNE activity titled Best Practices for Recognizing & Managing Immune-Related Adverse Events in the Emergency Department: Become Aware, Stay Alert, Change Your Practice, & Keep Patients With Cancer Safe. For the full presentation, monograph, complete CME/MOC/CNE information, and to apply for credit, please visit us at http://bit.ly/2MVl3DM. CME/MOC/CNE credit will be available until November 26, 2020.

Recommended
Recommended
More Related Content
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Best Practices for Recognizing & Managing Immune-Related Adverse Events in the Emergency Department: Become Aware, Stay Alert, Change Your Practice, & Keep Patients With Cancer Safe
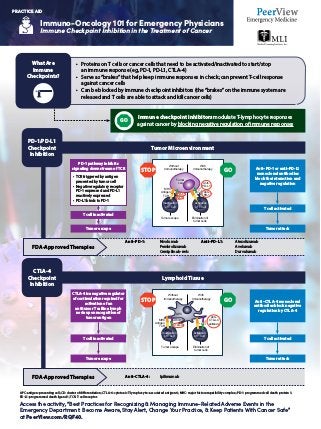
- 1. Immuno-Oncology 101 for Emergency Physicians Immune Checkpoint Inhibition in the Treatment of Cancer Access the activity, “Best Practices for Recognizing & Managing Immune-Related Adverse Events in the Emergency Department: Become Aware, Stay Alert, Change Your Practice, & Keep Patients With Cancer Safe” at PeerView.com/RQF40. PRACTICE AID APC: antigen-presenting cell; CD: cluster of differentiation; CTLA-4: cytotoxic T-lymphocyte–associated antigen 4; MHC: major histocompatibility complex; PD-1: programmed cell death protein 1; PD-L1: programmed death ligand 1; TCR: T-cell receptor. Tumor Microenvironment Lymphoid Tissue Immune checkpoint inhibitors modulate T-lymphocyte responses against cancer by blocking negative regulation of immune responses PD-1 pathway inhibits signaling downstream of TCR • TCR triggered by antigen presented by tumor cell • Negative regulatory receptor PD-1 expressed and PD-L1 reactively expressed • PD-L1 binds to PD-1 T cell inactivated T cell inactivated T cell activated T cell activated Anti–PD-1 or anti–PD-L1 monoclonal antibodies block the interaction and negative regulation Anti–CTLA-4 monoclonal antibodies block negative regulation by CTLA-4 CTLA-4 is a negative regulator of costimulation required for activation of an antitumor T cell in a lymph node upon recognition of tumor antigen PD-1/PD-L1 Checkpoint Inhibition CTLA-4 Checkpoint Inhibition FDA-Approved Therapies FDA-Approved Therapies Without Immunotherapy With Immunotherapy MHC Antigen TCR PD-1 PD-L1 Anti– PD-L1 Anti– PD-1 Tumor cell Tumor escape Inactivation of T Cell Activation of T Cell Elimination of tumor cells Without Immunotherapy With Immunotherapy MHC CD80/86 CTLA-4 Anti– CTLA-4 antibody APC Antigen TCR Inactivation of T Cell Activation of T Cell Tumor escape Elimination of tumor cells STOP STOP GO GO GO Tumor escape Tumor escape Tumor attack Tumor attack Anti–PD-1: Nivolumab Pembrolizumab Cemiplimab-rwlc Anti–CTLA-4: Ipilimumab Anti–PD-L1: Atezolizumab Avelumab Durvalumab • Proteins on T cells or cancer cells that need to be activated/inactivated to start/stop an immune response (eg, PD-1, PD-L1, CTLA-4) • Serve as “brakes” that help keep immune responses in check; can prevent T-cell response against cancer cells • Can be blocked by immune checkpoint inhibitors (the “brakes” on the immune system are released and T cells are able to attack and kill cancer cells) What Are Immune Checkpoints?
- 2. Immuno-Oncology 101 for Emergency Physicians Immune-Related Adverse Events in Patients With Cancer Access the activity, “Best Practices for Recognizing Managing Immune-Related Adverse Events in the Emergency Department: Become Aware, Stay Alert, Change Your Practice, Keep Patients With Cancer Safe” at PeerView.com/RQF40. PRACTICE AID What Are irAEs? • Immune checkpoint inhibitors are associated with important clinical benefits, but general immunologic enhancement can also lead to a unique spectrum of immune-related adverse events (irAEs) • Pathophysiology of irAEs is not entirely clear, but T-cell, antibody, and cytokine responses may be involved • irAEs differ significantly from toxicities of chemotherapies and other cancer therapies • Any organ system can be affected, but more commonly occurring irAEs are pulmonary (pneumonitis), dermatologic (rash, pruritus, blisters, ulcers, vitiligo), gastrointestinal (diarrhea, enterocolitis, transaminitis, hepatitis, pancreatitis), and endocrine (thyroiditis, hypophysitis, adrenal insufficiency) irAEs • irAEs can have unpredictable onset and can present at any time, but typically start within the first few weeks to months after treatment initiation and can occur after treatment discontinuation • irAEs can be difficult to differentiate from other etiologies and are often diagnosed by exclusion; other causes should be ruled out, but immunotherapy-related toxicity should always be included in the differential for patients who are receiving or have received immunotherapies Musculoskeletal Gastrointestinal Renal Hematologic Neurologic Pulmonary Cardiovascular Ocular Dermatologic Endocrine Spectrum of Potential irAEs Neuropathy, meningitis, Guillain–Barré syndrome, myasthenia gravis, encephalitis, and transverse myelitis Myocarditis, pericarditis, arrhythmias, impaired ventricular function with heart failure and vasculitis, and venous thromboembolism Pneumonitis Colitis, hepatitis, and hepatic transaminases Inflammatory arthritis, myositis, and polymyalgia-like syndrome Uveitis/iritis, episcleritis, and blepharitis Primary hypothyroidism, hyperthyroidism, hypophysitis, primary adrenal insufficiency, and diabetes Rash/inflammatory dermatitis, bullous dermatoses, and severe cutaneous adverse reactions Autoimmune hemolytic anemia, aTTP, hemolytic uremic syndrome, aplastic anemia, lymphopenia, ITP, and acquired hemophilia Nephritis
- 3. Immuno-Oncology 101 for Emergency Physicians Immune-Related Adverse Events in Patients With Cancer Access the activity, “Best Practices for Recognizing Managing Immune-Related Adverse Events in the Emergency Department: Become Aware, Stay Alert, Change Your Practice, Keep Patients With Cancer Safe” at PeerView.com/RQF40. PRACTICE AID Change How You Approach the Evaluation, Diagnosis, and Management of Patients With Cancer in the Emergency Department! Ask about history of cancer treatment, including immunotherapy, from any patient with cancer presenting to an ED in an acutely unwell state Call the oncology care provider for any moderate or severe (grade 2 or higher) toxicity upon presentation to discuss treatment history, if toxicity could be caused by immunotherapy, and next steps Patients receiving immunotherapies are often given wallet cards listing their therapies à ask about that Simplify treatment decisions à consider corticosteroids for frontline management of immune-related toxicities in most cases Coordinate with the oncology care provider and other specialists, if possible Modify your differential diagnosis when a patient has received cancer immunotherapy à almost any inflammatory condition could be caused by immune checkpoint inhibitor therapy Avoid premature closure A multidisciplinary approach can boost the collective awareness of irAEs and help keep patients safe! History Consultation Diagnosis Management
- 4. Immuno-Oncology 101 for Emergency Physicians Immune-Related Adverse Events in Patients With Cancer Access the activity, “Best Practices for Recognizing Managing Immune-Related Adverse Events in the Emergency Department: Become Aware, Stay Alert, Change Your Practice, Keep Patients With Cancer Safe” at PeerView.com/RQF40. PRACTICE AID General Recommendations for Grading, Assessment, and Management of irAEs1 irAEs are often diagnosed by exclusion; other causes should be ruled out (including AEs of other therapies used), but immunotherapy-related toxicity should always be included in the differential There should be a high level of suspicion that new symptoms are treatment related; early recognition, evaluation, and treatment of irAEs plus patient education are essential for the best outcome Depending on the severity of an irAE, management may require corticosteroids or other immunosuppressive treatment and interruption or discontinuation of therapy If appropriate immunosuppressive treatment is used, patients generally recover from irAEs Grade 1 Asymptomatic; diagnostic changes only; continue immunotherapy Grade 2 Mild-to-moderate symptoms; grade 2 diagnostic abnormalities • Hold treatment; provide supportive care • Methylprednisolone 0.5-1.0 mg/kg/d until stable (or oral equivalent) If improving: transition to oral steroid at start of taper • Dose suggested: 60 mg prednisone daily x 2 wk • Taper over 4 wk or more to reduce recurrence of symptoms • May consider reinitiation of immunotherapy If progressing: treat as grade 3/4 • Consider hospitalization of patient; multidisciplinary evaluation of toxicity Grade 3/4 Discontinue immunotherapy (consider organ-specific algorithms; endocrine) • Hospitalization indicated • Methylprednisolone 1.0-2.0 mg/kg/d until stable Refractory If no improvement or progression, additional immunosuppressant treatment may be needed • Infliximab 5 mg/kg (except if contraindicated) • Mycophenolate mofetil 1 g twice daily • Cyclosporine or IV immunoglobulin Grade Assessment and Management
- 5. Immuno-Oncology 101 for Emergency Physicians Immune-Related Adverse Events in Patients With Cancer Access the activity, “Best Practices for Recognizing Managing Immune-Related Adverse Events in the Emergency Department: Become Aware, Stay Alert, Change Your Practice, Keep Patients With Cancer Safe” at PeerView.com/RQF40. PRACTICE AID Organ-Specific Summary of Presentation, Assessment, and Management of irAEs1 Pneumonitis SOB, DOE, cough, wheezing, chest pressure, increased oxygen requirement, hypoxia, and tachycardia O2 saturation levels, CT of chest; rule out progression of disease, lymphangitic spread, pulmonary embolism, and pleural effusion O2 support, bronchoscopy ± BAL, steroids, and antibiotic prophylaxis Colitis Abdominal cramping or pain, loose stools, and altered frequency of stools Rule out infectious causes; stool cultures; rule out perforation; abdominal CT and lactoferrin and calprotectin levels If steroid refractory: infliximab; antispasmodic, antidiarrheal, and fluid support Rash/skin Macules, papules, morbilliform, pruritus, eczema, psoriasis, vitiligo, bullous pemphigoid, Stevens-Johnson syndrome, and TEN syndrome Rule out other causes; total body exam (include mucous membranes); measure distribution and skin biopsy Topical moderate-to-high– dose steroids; IV steroids; consult dermatology and infectious disease; if mucosa, consult gynecology, ophthalmology, and urology; admission: burn unit Endocrine— adrenal insufficiency Nonspecific fatigue, sluggishness, anorexia, weight change, irritability, and feeling hot or cold More common with anti–PD-1; monitor ACTH and cortisol Corticosteroids (must start prior to any other hormone replacement) and stress dosing in trauma Endocrine— hypophysitis Headache, fatigue, and visual changes CMP, glucose, cortisol, ACTH, pituitary panel (TSH, FSH, LH, ACTH, and prolactin); testosterone/estradiol; and MRI of brain with sellar cuts Hormone replacement Endocrine— hyperthyroidism Tachycardia and irritability Monitor TSH and T4 Antithyroid: methimazole; beta-blockers Endocrine— hypothyroidism Severe fatigue, sluggishness, anorexia, and weight gain Monitor TSH and T4 Levothyroxine; usually permanent Endocrine— type 1 diabetes Thirst, psychosis, and change in level of consciousness Blood glucose Insulin System Signs Symptoms Assessment Management
- 6. Immuno-Oncology 101 for Emergency Physicians Immune-Related Adverse Events in Patients With Cancer Access the activity, “Best Practices for Recognizing Managing Immune-Related Adverse Events in the Emergency Department: Become Aware, Stay Alert, Change Your Practice, Keep Patients With Cancer Safe” at PeerView.com/RQF40. PRACTICE AID ALK: alkaline phosphatase; ANA: antinuclear antibodies; aTTP: acquired thrombotic thrombocytopenic purpura; BAL: broncho-alveolar lavage; CCP: cyclic citrullinated peptide; CK: creatinine kinase; CMP: comprehensive metabolic panel; CRF: corticotropin-releasing factor; CRP: C-reactive protein; CXR: chest X-ray; DOE: dyspnea on exertion; EMG: electromyography; ESR: erythrocyte sedimentation rate; FSH: follicle-stimulating hormone; irAE: immune-related adverse event; ITP: immune thrombocytopenia; LH: luteinizing hormone; LP: lumbar puncture; OT: occupational therapy; PD-1: programmed cell death protein 1; PT: physical therapy; RF: rheumatoid factor; RUQ: right upper quadrant; SOB: shortness of breath; TEN: toxic epidermal necrolysis. 1. NCCN Clinical Practice Guidelines in Oncology. Management of Immunotherapy-Related Toxicities. Version 2.2019. https://www.nccn.org/professionals/physician_gls/pdf/immunotherapy.pdf. Accessed October 14, 2019. Organ-Specific Summary of Presentation, Assessment, and Management of irAEs1 (Cont’d) Note: This irAE list is not all inclusive Hepatic Nausea, vague abdominal discomfort, RUQ pain, dehydration, jaundice, bleeding, bruising, dark skin, and drowsiness Liver enzymes (AST, ALT, ALK, total and direct bilirubin), liver ultrasound, GI consult, and rule out viral syndrome Hold hepatotoxic drugs; mycophenolate 2 mg/kg/d; if refractory: no infliximab Renal/nephritis Elevated serum creatinine, vague nausea, emesis, decreased urine output, blood in urine, and ankle swelling Serum creatinine and urinalysis; nephrology consult, renal ultrasound, and biopsy Limit nephrotoxic drugs, antibiotics, NSAIDs, and contrast dye; identify high-risk patients (CRF); and hydration Cardiac Chest pain, SOB, tachycardia, arrhythmias, VTE, fluid retention, pericarditis, myocarditis, effusion, and vasculitis ECG, echocardiogram, CXR, and cardiology consult Blood pressure support and heart rate regulation Neurologic Unusual weakness, numbness, peripheral neuropathy, autonomic neuropathy, altered gait, memory difficulties, seizures, aseptic meningitis, myasthenia gravis, Guillain-Barré, encephalitis, and transverse myelitis Neurology consult, MRI of brain to rule out CVA and brain metastases; MRI spine; LP; rule out infection Permanent discontinuation; rehab services; IV immunoglobulin Ocular Dry, scratchy eyes; vision changes; redness; inflammation; pain; iritis; uveitis; blepharitis; episcleritis; and conjunctivitis Rule out infection and consult with ophthalmology Lubricating eye drops; topical corticosteroid eye drops; decrease local irritants: contact lens, eye makeup, etc. Musculoskeletal Inflammatory arthritis, myositis, and polymyalgia-like syndrome Rheumatologic tests: autoimmune panel (ANA, RF, anti-CCP, ESR, CK, and CRP); imaging and EMG NSAIDs, corticosteroid joint injections, DMARDs, methotrexate, and PT/OT System Signs Symptoms Assessment Management