
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Blood supply,nerve supply and lymphatic drainage of the periodontium final
Similar to Blood supply,nerve supply and lymphatic drainage of the periodontium final (20)
Recently uploaded
Recently uploaded (20)
Blood supply,nerve supply and lymphatic drainage of the periodontium final
- 1. BLOOD SUPPLY, NERVE SUPPLY & LYMPHATIC DRAINAGE OF THE PERIODONTIUM DR.NEHA PRITAM 1sr Year MDS PGT Department of Periodontics HIDSAR
- 2. THE PERIODONTIUM The periodontium is defined as those tissues supporting and investing the tooth and consists of cementum, periodontal ligament (PDL), bone lining the alveolus (socket), and that part of the gingiva facing the tooth. Ten Cate's Oral Histology,Development,Structure and Function
- 3. The normal periodontium provides the support necessary to maintain teeth in function. Four principle components 1. Gingiva 2. Periodontal ligament 3. Cementum 4. Alveolar bone
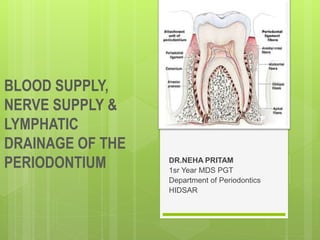
- 4. Fig.The anatomy of tooth with associated attachment apparatus
- 5. INTRODUCTION TO VASCULAR SUPPLY The orofacial structures have a very rich vascular supply. A very important artery that supplies the maxillary and mandibular teeth and their associated periodontium is the internal maxillary artery.
- 6. Internal maxillary artery The maxillary artery or the internal maxilary artery is one of the two terminal divisions of the external carotid artery. The second terminal branch being the superficial temporal artery
- 10. ARTERIAL SUPPLY OF MAXILLARY AND MANDIBULAR teeth and their supporting structures The mandibular teeth and their supporting structures are supplied by branches of inferior alveolar (dental) artery, including mental ,sublingual and buccal arteries. The artery supply of maxillary teeth and their supporting structure is by the posterior superior alveolar artery, infraorbital artery, the greater palatine artery and the sphenopalatine arteries.
- 11. Microcirculatory tracts, blood vessels, and lymphatic vessels play an important role in drainage of tissue fluid and in the spread of inflammation. In gingivitis and periodontitis, the microcirculation and vascular formation change greatly in the vascular network directly under the gingival sulcular epithelium and junctional epithelium.
- 12. Blood vessels are easily evidenced in tissue sections by means of immuno- histochemical reactions against proteins of endothelial cells (factor VIII and adhesion molecules). Before these techniques were developed, vascularization patterns of periodontal tissues had been described using histo- enzymatic reactions for alkaline phosphatase and adenosine triphosphatase because of the great activity of these enzymes in endothelial
- 14. The gingiva receives its arterial supply mainly from three sources: Supraperiosteal arteries Vessels of periodontal ligament Arterioles emerging from crests of interdental septa
- 15. Anatomic and histologic changes have been shown to occur In the gingival microcirculation with gingivitis. In the absence of inflammation, the vascular network is arranged in a regular, repetitive, and layered pattern. In contrast, the inflamed gingival vasculature exhibits an irregular vascular plexus pattern, with the microvessels exhibiting a looped, dilated, and convoluted appearance.
- 16. Beneath the epithelium on the outer gingival surface, capillaries extend into the papillary connective tissue between the epithelial rete pegs in the form of terminal hairpin loops with efferent and afferent branches ,spirals and varices.
- 17. Along the sulcular epithelium ,capillaries are arranged in a flat,anastomosing plexus that extents parallel to the enamel from the base of the sulcus to the gingival margin. In the col area,a mixed pattern of anastomosing capillaries and loops occurs.
- 19. Chronic periodontitis patients presented with increased recruitment of neutrophils to the oral cavity. Gene expression analysis revealed differences in the expression levels of genes from several biological pathways. The apoptosis network was significantly altered in patients with chronic inflammation in the oral cavity, with up-regulation of pro-survival members of the Bcl-2 family and down-regulation of pro-apoptosis members in the same compartment. The percentages of viable neutrophils are significantly increased in the oral cavity of chronic periodontitis patients. Lakschevitz FS, Aboodi GM, Glogauer M. Oral neutrophil transcriptome changes result in a pro-survival phenotype in periodontal diseases. PloS one. 2013 Jul 11;8(7):e68983.
- 21. VENOUS AND LYMPHATIC DRAINAGE The venous and lymphatic drainage of gingiva is closely related to the arterial supply. In the maxilla, the gingival lymphatic vessels drain into the deep cervical lymph nodes. In the mandible they drain into the mental,submandibular and cervical lymph nodes.
- 22. THE SUPERFICIAL AND DEEP CERVICAL LYMPH NODES
- 23. LYMPHATIC SYSTEM The lymphatic system is a network of lymph nodes are connected lymphatic vessels, which plays an important role in protecting the body from infection. The role of the lymphatic system is removing excess fluids, cellular and protein debris, microorganisms and other elements and is important in controlling diffusion and resolution of inflammatory process.
- 24. The lymphatic drainage of the gingiva brings in the lymphatics of the connective tissue papillae.It progresses into the collecting network external to the periosteum of the alveolar process, then to the regional lymph nodes, particularly the submaxillary group. In addition, lymphatics just beneath the junctional epithelium extend into the periodontal ligament and accompany the blood vessels.
- 26. The lymphatic system is a part of the overall lymphoid system of the body and a component of the immune system of the body. It is an accumulation of tiny channels or tubules with small nodular structures called lymph nodes interconnecting them. The system functions by returning fluids to the bloodstream from the various tissues of the body.
- 27. Gingival lymphatics are crucial for transcapillary fluid balance in the steady-state condition and during acute perturbation. Lymphangiogenesis takes place in gingiva during periodontal disease development. Moreover, gingival lymphatic vessels protect against P. gingivalis induced periodontitis, probably by enhancing clearance of bacterial products and promoting humoral immune responses. i
- 29. SOME OF THE MAJOR LYMPH NODE GROUPS IN THE HEAD AND NECK AREA Retropharyngeal nodes A group of nodes behind the throat wall and involved in throat infections. These nodes drain to the upper deep cervical lymph nodes.
- 30. FIG.LOCATION OF THE RETROPHARYNGEAL NODES WITH RELTAION TO THE PHARYNX AND THE SKULL BASE.
- 31. Submental nodes Found beneath the chin. The lymphatic channels from the mandibular incisors, the tip of the tongue, and the midline of the lower lip and chin drain into these nodes.
- 32. Submandibular nodes grouped around the submandibular gland near the angle of the mandible. The areas that drain into these nodes are all of the maxillary teeth, maxillary sinus, the mandibular canines and all mandibular posterior teeth; the floor of the mouth and most of the tongue; the cheek area; the hard palate; and the anterior nasal cavity.
- 34. Upper deep cervical nodes A number of nodes drain into this node-The submandibular nodes; the nodes behind the back throat wall, known as the retropharyngeal nodes; the parotid nodes in front of the ear and the parotid gland; and others drain into this.
- 35. Lower deep cervical nodes They drain the upper deep cervical nodes and many of the nodes at the back of the neck, frequently referred to as occipital nodes, as well as some glands in the anterior neck. From the lower deep cervical nodes, the lymphatic fluid drains into the junction of the subclavian and internal jugular veins.
- 37. SPREAD OF DISEASES BY LYMPH NODES The terms primary nodes, secondary nodes, and tertiary nodes are often used in discussions about infections and cancer, both of which spread through lymphatic channels. These terms refer to the groups of nodes that are affected in a disease process.
- 39. Infections originating in the middle of the lower lip would spread first to the submental nodes Secondarily to the submandibular nodes Then to the upper deep cervical nodes(which in this instant would be tertiary nodes of involvement)
- 40. An understanding of this concept is necessary to comprehend also the spread of oral cancer. Each group of nodes acts as a resistance barrier against the spread of cancer.
- 41. The nodes slow the spread, and if the cancer is detected early enough, it can be treated more successfully. Once the infection or the cancer reaches the lower deep cervical nodes and passes through them, it enters the bloodstream, moving directly into the heart and then throughout the body.
- 42. With this in mind, it is easy to understand why cancer on the tip of the tongue does not result in as high a mortality rate as does cancer that begins further back on the tongue or in the throat.
- 43. The tip of the tongue generally drains through four groups of nodes before it enters the bloodstream and spreads throughout the body, whereas cancer in the posterior portion of the tongue or in the throat travels to the upper deep cervical nodes, on to the lower deep cervical nodes, and into the bloodstream.
- 44. SPREAD OF INFECTIONS IN FASCIAL SPACES Another way through which infections may spread is through fascial spaces. Although infection spread through fascial spaces is much less common, it displays much more dramatic clinical symptoms.
- 45. The spaces between muscle and tissue layers are referred to as fascial layers or planes, and infections may spread here.
- 46. In general, dental infections start in the maxilla or mandible at the apex of a tooth or in the periodontal space around a tooth. Most periodontal space infections cause a swelling of the gingival or mucosal tissue within the oral cavity. Infections at the apices of the teeth cause swelling in one of two directions: buccal or lingual. Most buccal swellings also lead to a swelling in the vestibule of the oral cavity.
- 47. This swelling is sometimes referred to as a gumboil. The infection comes to a pointed head, breaks through the mucosa, and drains into the oral cavity.
- 49. Entry of infections into the buccal space is dependent on their relationship to the attachment of the buccinator muscle.
- 51. Infection spreading into the sublingual ,submandibular space causes a swelling into the floor of the mouth. If it spreads into the submental space, it will cause a swelling beneath the chin, sometimes referred to as Ludwig’s angina. These infections continue to spread by gravity if not treated.
- 52. The importance of this section is not to be able to completely describe or define the boundaries of these spaces or potential spaces, but to understand how the origin or location of the original infection determines the pathway it will follow and the potential outcome if left untreated.
- 53. MAXILLARY INFECTIONS If the infection does not open into the maxillary buccal vestibule or onto the palate, it may spread toward three areas—the nasal cavity, the maxillary sinus, or the soft- tissue spaces of the cheek or the area below the eye.
- 54. The area involved is related to the tooth involved. A swelling below the eye is usually related to infection from an anterior tooth, usually the maxillary canine, whereas swelling in the cheek is usually related to infection in a posterior tooth
- 55. NERVE SUPPLY
- 56. Neural elements are extensively distributed throughout the gingival tissues. Within the gingival connective tissues, most nerve fibers are myelinated and are closely associated with the blood vessels. Gingival innervation is derived from fibers arising from nerves in the periodontal ligament and from the labial, buccal, and palatal nerves. The following nerve structures are present in the connective tissue: a meshwork of terminal argyrophilic fibers, some of which extend into the epithelium; Meissner-type tactile corpuscles; Krause-type end bulbs, which are temperature receptors; and encapsulated spindles
- 57. The neural tissue in human periodontium is associated with the terminal part of a nerve trunk from which myelinated nerve fibres leave and in some instances divide into three or more nerve fibres.
- 58. Innervations in various regions of the oral cavity is supplied by the second and third divisions of the trigeminal nerve.
- 60. Innervations in various regions of the oral cavity is supplied by the second and third divisions of the trigeminal nerve. Trigeminal nerves have sensory, motor, and intermediate roots, which are mounted directly to the brain.
- 61. The nerve supply of gingiva follow the vascular supply. In the maxilla,the gingiva is supplied by the posterior ,middle and the anterior superior alvoelar nerves,branches of infraorbital nerves,the greater palatine nerve and nasopalatine nerve.
- 62. The middle superior alveolar nerve is present in 80% of individuals The buccal nerve supplies variably in the buccal molar region.
- 63. In the mandible,gingiva is largerly suplied by the inferior alveolar nerve. The buccal nerve supplies buccal gingiva in relation to molars and premolars. Branches of lingual nerve supplies the lingual aspect of all lower teeth.
- 65. REFERENCE Lakschevitz FS, Aboodi GM, Glogauer M. Oral neutrophil transcriptome changes result in a pro-survival phenotype in periodontal diseases. PloS one. 2013 Jul 11;8(7):e68983. Griffin CJ, Harris R. Innervation of human periodontium I. Classification of periodontal receptors. Australian dental journal. 1974 Feb;19(1):51-6. Carranza’s clinical periodontology Newman Takei Klokkevoid Carranza Ten Cate’s Oral Histology Developent Structure and Function
- 66. CONCLUSION A thoughrough understanding of the anatomical structures,vasculature and innervations of the periodontium is necessary for the clinical point of view and before making any surgical intervention in this area.
Editor's Notes
- Proper functioning of the periodontium is achieved only through structural integrity and interaction between these various tissues.
- Periodontal diseases are inflammatory processes that occur following the influx of neutrophils into the periodontal tissues in response to the subgingival bacterial biofilm. Current literature suggests that while neutrophils are protective and prevent bacterial infections, they also appear to contribute to damage of the periodontal tissues. In the present study we compare the gene expression profile changes in neutrophils as they migrate from the circulation into the oral tissues in patients with chronic periodontits and matched healthy subjects. We hypothesized that oral neutrophils in periodontal disease patients will display a disease specific transcriptome that differs from the oral neutrophil of healthy subjects. Venous blood and oral rinse samples were obtained from healthy subjects and chronic periodontitis patients for neutrophil isolation. mRNA was isolated from the neutrophils, and gene expression microarray analysis was completed. Results were confirmed for specific genes of interest by qRT-PCR and Western Blot analysis.