1. INTRODUCTION
Breast cancer is the most feared disease amongst women (Ganz, 2000) and is ranked the fifth cause of death
globally of women both in the developed and developing world (Bridges et al., 2011). Regional research reveals
that there has been a steady increase in breast cancer in the Middle East and Asian regions over the last three
decades, with Arab woman being afflicted ten years younger, on average, than in the West (Brown et al., 2012).
Higher mortality can be equated to lifestyle changes and economics, which has seen dramatic effects to health
(Brown et al., 2012). Complex issues such as exacerbated diagnostic and treatment costs, cultural factors, habits
of education and awareness have been brought to the attention at a regional level.
The Gulf region as a whole needs to address specific needs of its population, whilst taking into account regionally
sensitive cultural nuances which can help to reduce disparities within healthcare provision. With a low public
awareness coupled with high misconceptions regarding breast cancer, effective healthcare strategies and
initiatives are needed to improve care within the Gulf region.
AIMS
To describe and investigate the lived experiences of Arab women with breast cancer
To identify the support from the participants perspectives that are necessary to support breast cancer patients
in Bahrain
To contribute to a deeper understanding of these experiences and of how they shape the lives of women with
breast cancer in Bahrain
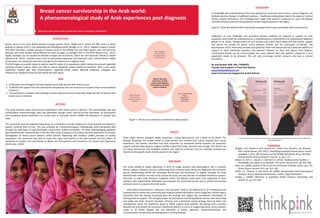
RESULTS
Three major themes emerged: Bodily Awareness, Coping Mechanisms and a Need to be Heard. The
findings illustrated the unique needs of Arab women and showed how culture shaped their cancer
experience. The women described how they depended on immediate family members for emotional
support and how they drew on religious beliefs to give them hope, direction and courage. This distinct set
of coping mechanisms and strategies evidence the need for protocols that are culturally sensitive and
tailored to the specific needs of Arab women in the region
DISCUSSION
The issues related to bodily awareness in term of image, physical and psychological, was a common
theme. Support networks are key in addressing other inherent issues during the diagnostic and treatment
phases. Relationships within the immediate family were the foundation of support amongst the Arab
literature and could be not only to the cultural structure, but also the lack of available healthcare support.
Dissimilar to other Arab literature, husbands within the Bahrain study were truly supportive of their
partners, with stigmatisation addressed more towards the unmarried women due to cultural and societal
pressure, which is unique to the Arab world.
Information dissemination, awareness and education need to be addressed at an institutional and
national level to inform the community with evidence based information, and to dispel the cultural taboos
associated with the disease. Surprising were the findings that religion was considered a foundation or
starting point of support. The strengths drawn by participants from being Muslim women was astounding
and unlike any other research reviewed. Utilising such a dominant coping strategy must be taken into
consideration within the healthcare arena to better support Arab patients. Harnessing such a positive
attitude will only benefit all concerned. Healthcare delivery in terms of supporting breast cancer patients
needs to be better aligned and not fractional. A holistic approach, interprofessionalism and
communication are key areas of development in moving forward..
CONCLUSION
A knowledge and understanding of the lived experiences of women who survive a cancer diagnosis can
facilitate positive change in healthcare practices. Healthcare professionals need to be aware of cultural
factors, coping mechanisms and strategies that shape Arab women’s responses to care and develop
culturally sensitive protocols and guidelines to best support women in the region
Figure 2- Think Pink Bahrain 2012 advertising campaign both Arabic and English with local discourse
Integration of such challenges and innovative delivery methods are required to support an Arab
population and should be underpinned by a multidisciplinary, multicentred and multinational approach
(Brown et al., 2012). Transformation of care services that match these needs will only further support
and reduce the burden for breast cancer patients, families and the community of Bahrain. The
development of the information booklet sponsored by Think Pink Bahrain will be a welcome addition of
support to both healthcare providers and patients. Reliance on facts and figures from Western
counterparts should not be communicated but more relevant data and statistics related to a local
population needs to be amassed. This will only encourage further research and have a cultural
foundation.
By Julie Sprakel; RGN, MSc, FFNMRCSI
Founder and President of Think Pink Bahrain
www.thinkpinkbahrain.com
Head of Community Engagement at RCSI Bahrain
** this research was undertaken as part of a MSc in part funded by the RCSI Bahrain as part of their professional
development policy **
REFERENCES
Bridges, J.F.P., Anderson, B.O., Buzaid, A.C., Jazieh, A.R., Niessen, L.W., Blauvelt,
B.M. and Buchanan, D.R. (2011). Identifying important breast cancer control
strategies in Asia, Latin America and the Middle East/North Africa. Bio Med
Central Health Services Research. Sep 20; 11. pp: 1-13.
Brown, R., Kerr, K., Haoudi, A. and Darzi, A. (2012). Tackling cancer burden in
the Middle East: Qatar as an example. The Lancet. Nov;13 (11). pp: 501-508.
Ganz, P.A. (2000). Quality of life across the continuum of breast cancer care. The
Breast Cancer Journal. 6 (5). pp: 324- 330.
Smith, J.A., Flowers, P. and Larkin, M. (2009). Interpretative Phenomenological
Analysis: Theory, Method and Research. London, Sage Publications.
Yardley, L. (2000). Dilemmas in qualitative health research. Psychology and
Health. 15. pp: 215-228.
METHODS
This study explored seven Arab women’s experiences with breast cancer in Bahrain. The methodology used was
Interpretative Phenomenology. Data was generated through seven semi-structured interviews. All participants
had completed clinical treatments six month prior to interview. Smith’s (2009) IPA framework of analysis was
used.
The researcher used the explored experiences as a method to provide evidence to move forward and address a
patient centered level of care. This was achieved by a phenomenological methodology which generated data
through the interviews of each participant using Smith’s (2009) framework. The (IPA) methodological approach
was selected by the researcher due to the fact that mode of enquiry is to analyse the lived experience of a certain
demographic of breast cancer patients within Bahrain. Operating with Yardley’s (2000) principles of quality
assessment, the researcher was able to assess the rigour and quality of the said research via four pillars; (i)
Sensitivity to Context, (ii) Commitment to Rigour, (iii) Transparency and Coherence, (iv) Impact and Importance
(Smith et al., 2009).
Breast cancer survivorship in the Arab world:
A phenomenological study of Arab experiences post diagnosis
What is the lived
experience of Arab
women post diagnosis
and treatment of breast
cancer in Bahrain
BODILY AWARENESS
Physical symptoms
Psychological symptoms
Altered Body Image
COPING MECHANISMS
Religion
Bargaining Tool
Social Support
Arab Culture
NEED TO BE HEARD
Healthcare Facilities
Awareness & Education
Information
Figure 1- Themes and subthemes revealed from data analysis