3. N. Kekenadze, MD, PhD
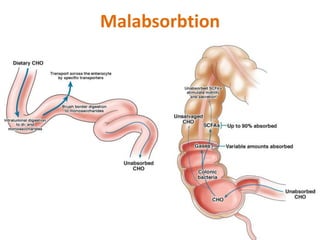
Malabsorption describes a
malfunction of the intestinal wall,
resulting in the insufficient
absorption of breakdown
products.
Malabsorption disorders can be
caused by either the insufficient
absorption or digestion
of nutrients.
4. N. Kekenadze, MD, PhD
Malasorbtion
Global malabsorption: in diseases
causing diffuse mucosal damage or a
reduction of the absorptive surface
(e.g., celiac disease)
Partial malabsorption: caused by a
localized absorption impairment,
resulting in deficiencies of
specific nutrients (e.g., vitamin
B12 deficiency in patients with diseases
affecting the terminal ileum)
5. N. Kekenadze, MD, PhD
Maldigestion
• Exocrine pancreatic insufficiency
• Definition: inability of the pancreas to produce enzymes
necessary for digestion, including amylase, lipases,
and proteases (e.g., trypsinogen, chymotrypsinogen, elastase)
• Etiology
– Cystic fibrosis
– Chronic pancreatitis
– Obstruction (e.g., due to pancreatic cancer)
– Shwachman-Diamond syndrome: rare autosomal recessive condition
and second most common cause of exocrine pancreatic
insufficiency in children (after cystic fibrosis)
• Gastric resection: lack of gastric acid → impaired breakdown
of nutrients
• Bile acid deficiency: e.g., cholestasis, bile
acid malabsorption → incomplete emulsification of fats
• Medications: orlistat
6. N. Kekenadze, MD, PhD
Malasorbtion
• Inflammatory bowel disease (e.g., Crohn's disease)
• Celiac disease (gluten-sensitive enteropathy)
• Infections (e.g.,tropical sprue, giardiasis, traveler's diarrhea, Whipple's
disease)
• Lactose intolerance
• Small intestine resection (short bowel syndrome)
– Definition: a condition in which the small intestine is unable to adequately
absorb nutrients, water, and electrolytes
– Etiologies: surgical resection (e.g., for Crohn disease or trauma), congenital
abnormalities
– Complications: intestinal failure that requires intravenous supplementation
• Chronic mesenteric ischemia
• Radiation colitis
• Impaired intestinal lymphatic circulation
• Hormonally active tumors (gastrinoma, VIPoma, carcinoid tumors)
• Small intestinal bacterial overgrowth (SIBO; blind loop syndrome)
• HIV enteropathy
7. N. Kekenadze, MD, PhD
Clinical features
• General symptoms
• Global malabsorption
– Diarrhea (most common), steatorrhea, abdominal distention,
flatulence
– Weight loss, fatigue
– Additional symptoms of specific deficiencies
• Partial (isolated) malabsorption: only symptoms specific to
individual nutrient deficiencies (e.g.,
impaired cobalamin absorption with megaloblastic anemia)
• Deficiencies
• Deficiency of fat-soluble vitamins
• Deficiency of water-soluble vitamins
• Zinc deficiency
• Protein: edema, cachexia
• Iron deficiency anemia or microcytic anemia
• Electrolytes: hypokalemia or hypocalcemia
8. N. Kekenadze, MD, PhD
Diagnostics
• Blood tests: macrocytic and/or microcytic anemia; ↓ electrolytes, ↓ total
protein, vitamin deficiencies
• Stool tests
– Analysis of fecal fat over 72 hours (e.g., using Sudan stain)
– Detection of pathogens
• D-xylose absorption test: assesses the absorptive function of the
upper small intestine
– Interpretation
• ↓ D-xylose levels (urine and blood) occur in malabsorptive disorders that involve damage to
the intestinal mucosa (e.g., celiac disease, Whipple disease) and in cases of bacterial
overgrowth.
• Normal (elevated) D-xylose levels suggest a different cause of malabsorption.
• Hydrogen breath test: assess the intestinal absorption of
individual carbohydrates
– Lactulose breath test: determination of orocecal transit time (small intestine transit
time) [1]
– Glucose hydrogen breath test: if abnormal bacterial colonization of the small
intestine is suspected
• Further testing (for underlying diseases): e.g., celiac disease or lactose
intolerance
9. N. Kekenadze, MD, PhD
Treatment
• Symptomatic treatment
• Oral supplementation
of fluid, nutrients, and vitamins
• Calorie and protein-enriched diet
• IV nutrition in severe cases (e.g.,
following extensive intestinal
resection)
• Causal treatment of the underlying
disease
10. N. Kekenadze, MD, PhD
Celiac disease
(Gluten-sensitive enteropathy, Nontropical sprue)
Characterized by:
maladaptive immune
response to gluten, a protein
found in many grains (e.g.,
wheat), villous atrophy Crypt
hyperplasia, therefore, a
disorder of absorption in the
small intestine, especially in
the upper part.
11. N. Kekenadze, MD, PhD
Epidemiology
• Sex: ♀ > ♂
• Age of onset
– The disease can occur at any age.
– Peak incidence is bimodal:
• At 8–12 months (or 2–3 months following the first exposure
to gluten through diet containing wheat)
• Third to fourth decade of life
• Prevalence: in the US ∼ 1:150 [2]
• Race: more common in individuals of northern
European descent
12. N. Kekenadze, MD, PhD
Etiology
• Genetic predisposition with association
to HLA antigens [3]
– HLA-DQ2 in 90–95% of patients
– HLA-DQ8 in 5–10% of patients
• Consuming gliadin from grains such as wheat, rye,
and barley leads to an autoimmune reaction within
the small intestinal wall.
• Commonly associated with autoimmune diseases
13. N. Kekenadze, MD, PhD
Clinical features
• Gastrointestinal symptoms
• Chronic or recurring diarrhea: steatorrhea
• Flatulence, abdominal bloating, and pain
• Nausea/vomiting
• Lack of appetite
• Constipation (rarely)
• Extraintestinal symptoms and associations
• Malabsorption symptoms: fatigue, weight
loss, vitamin deficiency, iron deficiency anemia, osteoporosis, hypocalcemia
• In children: failure to thrive, growth failure, delayed puberty
• Dermatologic associations: dermatitis herpetiformis
• Neuropsychiatric symptoms: peripheral neuropathies (numbness, burning and
tingling of the hands and feet) , headache, ataxia, depression, irritability [4]
• Gynecological associations: reduced fertility or infertility
• Endocrine associations: autoimmune thyroid disease, type 1 diabetes mellitus
• Associated chromosomal syndromes: Turner syndrome, Down syndrome
• Other associated conditions: autoimmune hepatitis, inflammatory bowel
disease, rheumatoid arthritis, sarcoidosis, selective IgA deficiency
15. N. Kekenadze, MD, PhD
Diagnostics
• Laboratory studies
• IgA tissue transglutaminase antibody (tTG IgA): initial
test, widely available test with sensitivity and specificity ≥
95%
• Total IgA - is common in its deficiency
• HLA – Testing
• Anti-endomysial antibody (EMA): Potential second-
line confirmatory test (high-specificity)
• Endoscopy [3][6]
• EGD with small intestine biopsy (confirmatory test)
• At least five duodenal biopsies should be taken (with ≥
1 from the duodenal bulb
• Crypt hyperplasia
• Villous atrophy
17. N. Kekenadze, MD, PhD
Treatment
• Diet
• Strict, lifelong gluten-free diet
– Abstain from products containing wheat, rye, barley, or spelt.
– Symptoms usually improve quickly Recommended foods: rice,
corn, potatoes, soybeans, millet
• Patients with secondary lactase deficiency: Avoid milk
products.
• Other
• Iron and vitamin supplementation, if there are
deficiencies (e.g., iron deficiency anemia)
• Consider osteoporosis screening in adult patients
• Refer patients to a dietitian and advise joining support
groups.
18. N. Kekenadze, MD, PhD
Complications
• Secondary lactase deficiency
• Moderately increased risk of malignancies
– Enteropathy-associated T-cell lymphoma (EATL)
– Adenocarcinoma of the small bowel
– Esophageal cancer [20]
• Refractory celiac disease (RCD): persistence and
worsening of celiac symptoms despite strict
adherence to gluten-free diet for 12 months
– May lead to ulcerative jejunitis
– In severe cases, total parenteral nutrition and treatment
with steroids or immunosuppressants may be necessary.
19. N. Kekenadze, MD, PhD
Whipple disease
• Definition: an infectious disease caused by Tropheryma whipplei,
an intracellular gram-positive bacteria
• Epidemiology
– Very rare
– Most commonly occurs in males older than 40 years [17][18]
• Clinical features
– Intestinal manifestations
• Abdominal pain
• Malabsorption syndrome (including diarrhea and/or steatorrhea): commonly occurs
later in the disease progression
– Extraintestinal manifestations
• Enteropathic arthritis (60% of cases)
• Arthralgias and arthritis, especially sacroiliitis (40% of cases)
• Fever
• Hyperpigmentation affecting sun-exposed areas
• Polyserositis
• Lymphadenopathy
• Cardiac symptoms (e.g., valve insufficiencies)
• Neurological symptoms (e.g., myoclonia, ataxia, impairment of oculomotor
function)
20. N. Kekenadze, MD, PhD
Diagnostics
– Small intestine biopsies: detection of PAS-
positive foamy macrophages in the lamina propria
• If gastrointestinal symptoms are absent, biopsies may also be
taken from other sites with disease activity
– PCR testing and immunohistochemistry staining
– Imaging may show enlarged mesenteric nodes.
– If neurological complaints occur: Perform a lumbar
puncture and CSF analysis and neuroimaging (MRI).
• Treatment
– IV ceftriaxone for 2 weeks
– Maintenance treatment with oral trimethoprim-
sulfamethoxazole for 1 year
21. N. Kekenadze, MD, PhD
Small intestinal bacterial overgrowth (SIBO)
• Definition: a pathologically increased growth of bacteria in the small intestine
• Etiology
• Anatomic causes
• Short bowel syndrome
• Blind loop syndrome: bacterial overgrowth in the bypassed intestinal segment (blind loop) that occurs
as a result of gastrectomy
• Small bowel diverticulosis
• Inflammatory bowel disease
• Motility disorders
• Irritable bowel syndrome
• Diabetes mellitus
• Scleroderma
• Pathophysiology: all resulting from bacterial overgrowth [55]
• ↓ Absorption of vitamin B12, fat-soluble vitamins, zinc, and iron
• ↑ Production of folate
• ↑ Deconjugation of the bile acids
• Clinical features
• Diarrhea, steatorrhea
• Abdominal discomfort, flatulence
• Weight loss, malabsorption
• Diagnostics [56]
• Jejunal aspirate cultures collected during endoscopy
• Positive lactulose breath test
• Management
• Antibiotic therapy
• Parenteral supplementation of vitamins and proteins
• In some cases, surgical treatment
22. N. Kekenadze, MD, PhD
Protein-losing enteropathy
• Etiology
– Massive loss of protein caused by various gastrointestinal
disorders
– Erosive or ulcerative (e.g., Crohn's disease, clostridium difficile
infection)
– Increased intestinal permeability to proteins (e.g., celiac
disease, bacterial overgrowth)
– Impaired lymphatic circulation (e.g., intestinal
lymphangiectasia, Whipple's disease)
• Clinical
features: hypoalbuminemia with peripheral edema
– In cases of systemic diseases, symptoms may be those of the
underlying condition.
– Further gastrointestinal symptoms may occur depending on the
underlying disorder.
• Treatment: treatment of the underlying disease
23. N. Kekenadze, MD, PhD
A 42-year-old man comes to the physician because he is
concerned that he is balding. Over the past few months,
he has noticed patchy areas of hair loss on his head. He
also mentions that he has felt depressed since the death
of his wife last year and has unintentionally lost about 18
kg (40 lb). He is constantly fatigued. He has little appetite
because he feels food does not taste the same way
anymore. He also has occasional episodes of watery
diarrhea. He drinks 5–6 cans of beer daily. Vital signs are
within normal limits. Examination shows dry, scaly skin
on both feet. There is patchy alopecia of the scalp,
axillae, chest, and mons pubis. Which of the following is
most likely to improve this patient's alopecia?
24. N. Kekenadze, MD, PhD
• A previously healthy 20-year-old woman comes to the
physician because of recurrent abdominal cramps, bloating,
and diarrhea for 4 months. She describes her stools
as greasy, foul-smelling, and difficult to flush. During this
time she has had a 6-kg (13.2-lb) weight loss. She has no
personal or family history of serious illness. Physical
examination shows pallor and cheilitis. Laboratory studies
show a hemoglobin concentration of 11 g/dL. Serum
concentrations of electrolytes, urea nitrogen, and
creatinine are within the reference range. Test of the stool
for occult blood is negative and stool microscopy reveals no
pathogens and no leukocytes. Analysis of a 24-hour stool
sample shows 12 g of fat. The patient is asked to
consume 25 g of d-xylose. Five hours later, its concentration
is measured in urine at 2 g (N = > 4 g/5 h). The test is
repeated after a two-week course of rifaximin, but
the urinary concentration of d-xylose remains the same.
Which of the following is the most likely diagnosis?
25. N. Kekenadze, MD, PhD
Eight weeks after starting a new weight-loss medication,
a 43-year-old woman with obesity comes to the
physician because of greasy diarrhea, excessive belching,
and flatulence. She also complains of progressively
worsening night-time vision. She has had no fever, chills,
or vomiting. Physical examination shows dry, scaly skin
on her extremities and face. Which of the following is the
most likely mechanism of action of the drug she is
taking?
26. N. Kekenadze, MD, PhD
• A 48-year-old man comes to the physician because of severe joint pain and
swelling involving different joints for 3 months. He has also been having loose
stools and episodes of epigastric pain for 6 months. He reports a 10-kg (22-lb)
weight loss during this period. He has type 2 diabetes mellitus. He does not smoke
or drink alcohol. His medications include insulin and metformin. His vital signs are
within normal limits. Examination shows pale conjunctivae, angular cheilitis, and
glossitis. Axillary and cervical lymphadenopathy is present. A grade
2/6 pansystolic murmur is heard best at the apex. The right knee is swollen and
tender; range of motion is limited. The sacroiliac joints are tender. Test of the stool
for occult blood is negative. Laboratory studies show:
Hemoglobin 9.2 g/dL
Mean corpuscular volume 90 μm3
Leukocyte count 4800/mm3
Serum
Na+ 134 mEq/L
Cl- 96 mEq/L
K+ 3.3 mEq/L
Glucose 143 mg/dL
Creatinine 1.2 mg/dL
A small intestine biopsy shows periodic acid-Schiff-positive (PAS-positive)
macrophages in the lamina propria. Which is the most appropriate next step in
management?