1. CRU1
05-2013
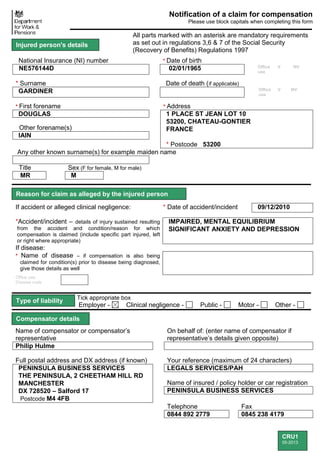
Notification of a claim for compensation
Please use block capitals when completing this form
All parts marked with an asterisk are mandatory requirements
as set out in regulations 3,6 & 7 of the Social Security
(Recovery of Benefits) Regulations 1997
National Insurance (NI) number * Date of birth
NE576144D 02/01/1965 Office
use
V NV
* Surname Date of death (if applicable)
GARDINER Office
use
V NV
* First forename * Address
DOUGLAS 1 PLACE ST JEAN LOT 10
53200, CHATEAU-GONTIER
FRANCE
* Postcode 53200
Other forename(s)
IAIN
Any other known surname(s) for example maiden name
Title Sex (F for female, M for male)
MR M
If accident or alleged clinical negligence: * Date of accident/incident 09/12/2010
*Accident/incident – details of injury sustained resulting
from the accident and condition/reason for which
compensation is claimed (include specific part injured, left
or right where appropriate)
IMPAIRED, MENTAL EQUILIBRIUM
SIGNIFICANT ANXIETY AND DEPRESSION
If disease:
* Name of disease – if compensation is also being
claimed for condition(s) prior to disease being diagnosed,
give those details as well
Office use:
Disease code
Tick appropriate box
Employer - Clinical negligence - Public - Motor - Other -
Name of compensator or compensator’s
representative
On behalf of: (enter name of compensator if
representative’s details given opposite)
Philip Hulme
Full postal address and DX address (if known) Your reference (maximum of 24 characters)
PENINSULA BUSINESS SERVICES
THE PENINSULA, 2 CHEETHAM HILL RD
MANCHESTER
DX 728520 – Salford 17
Postcode M4 4FB
LEGALS SERVICES/PAH
Name of insured / policy holder or car registration
PENINSULA BUSINESS SERVICES
Telephone Fax
0844 892 2779 0845 238 4179
Injured person's details
Compensator details
Reason for claim as alleged by the injured person
Type of liability
2. CRU USE STB IS DLA PIP Scrutinised by
BPO ESA JSA AA UC ………………
DISB DWA
CRU1
05-2013
Name of representative Reference (maximum of 24 characters)
Full postal address and DX address (if known) Telephone
Postcode
Fax
Did the injured person receive NHS treatment because of the
incident?
*Yes No Not Yet Known
Is the compensator the same as the Trust? *Yes No
(If yes do not complete hospital details)
Details of the hospital(s) the injured person attended or admitted to in order of attendance.
* Name of hospital (1) (if applicable) Name of hospital (2) (if applicable)
* Address (if applicable) Address
Postcode Postcode
For Road Traffic accidents before 29.01.07:If you are claiming exemption from recovery of NHS charges
on the grounds of nil requirement to carry compulsory insurance, (section 144, Road Traffic Act 1988)
state category of exemption here:
Only complete in disease cases or if date of accident is before 06.04.1994
Was the injured person absent from work prior to 06.04.1994 as a result
of the disease/condition(s) for which compensation has been claimed? Yes No
If yes, please give name and address of employer(s) and employee payroll number here:
Send this form to: Compensation Recovery Unit DX68560
Durham House Washington 4
Washington
Tyne & Wear Fax: 0191 2252324
NE38 7SF
email: cru1@dwp.gsi.gov.uk Date: 16/05/2014
All parts marked with an asterisk are mandatory requirements
as set out in Regulation 7 of the Road Traffic (NHS Charges)
Regulations 1999 and Regulation 5 of the Personal Injuries
(NHS Charges) (General) and Road Traffic (NHS Charges)
(Amendment) Regulations 2006
Injured person's representative details
Employment details
What to do now
Hospital details
All incidents on or after 29.01.07
Road Traffic Accidents only before 29.01.07
3. CRU1
05-2013
Notification of a claim for compensation
Please use block capitals when completing this form
All parts marked with an asterisk are mandatory requirements
as set out in regulations 3,6 & 7 of the Social Security
(Recovery of Benefits) Regulations 1997
National Insurance (NI) number * Date of birth
NE576144D 02/01/1965 Office
use
V NV
* Surname Date of death (if applicable)
GARDINER Office
use
V NV
* First forename * Address
DOUGLAS 1 PLACE ST JEAN LOT 10
53200, CHATEAU-GONTIER
FRANCE
* Postcode 53200
Other forename(s)
IAIN
Any other known surname(s) for example maiden name
Title Sex (F for female, M for male)
MR M
If accident or alleged clinical negligence: * Date of accident/incident 09/12/2010
*Accident/incident – details of injury sustained resulting
from the accident and condition/reason for which
compensation is claimed (include specific part injured, left
or right where appropriate)
IMPAIRED, MENTAL EQUILIBRIUM
SIGNIFICANT ANXIETY AND DEPRESSION
If disease:
* Name of disease – if compensation is also being
claimed for condition(s) prior to disease being diagnosed,
give those details as well
Office use:
Disease code
Tick appropriate box
Employer - Clinical negligence - Public - Motor - Other -
Name of compensator or compensator’s
representative
On behalf of: (enter name of compensator if
representative’s details given opposite)
Patrick Mcbrien Exsto Uk & Ors
Full postal address and DX address (if known) Your reference (maximum of 24 characters)
DWF LLP
1 SCOTT PLACE, 2 HARDMAN STREET
MANCHESTER
DX 14313 – MANCHESTER
Postcode M3 3AA
PMB/PXB/2006751-334
Name of insured / policy holder or car registration
EXSTO
Telephone Fax
01225 703329 01225 791905
Injured person's details
Compensator details
Reason for claim as alleged by the injured person
Type of liability
4. CRU USE STB IS DLA PIP Scrutinised by
BPO ESA JSA AA UC ………………
DISB DWA
CRU1
05-2013
Name of representative Reference (maximum of 24 characters)
Full postal address and DX address (if known) Telephone
Postcode
Fax
Did the injured person receive NHS treatment because of the
incident?
*Yes No Not Yet Known
Is the compensator the same as the Trust? *Yes No
(If yes do not complete hospital details)
Details of the hospital(s) the injured person attended or admitted to in order of attendance.
* Name of hospital (1) (if applicable) Name of hospital (2) (if applicable)
* Address (if applicable) Address
Postcode Postcode
For Road Traffic accidents before 29.01.07:If you are claiming exemption from recovery of NHS charges
on the grounds of nil requirement to carry compulsory insurance, (section 144, Road Traffic Act 1988)
state category of exemption here:
Only complete in disease cases or if date of accident is before 06.04.1994
Was the injured person absent from work prior to 06.04.1994 as a result
of the disease/condition(s) for which compensation has been claimed? Yes No
If yes, please give name and address of employer(s) and employee payroll number here:
Send this form to: Compensation Recovery Unit DX68560
Durham House Washington 4
Washington
Tyne & Wear Fax: 0191 2252324
NE38 7SF
email: cru1@dwp.gsi.gov.uk Date: 16/05/2014
All parts marked with an asterisk are mandatory requirements
as set out in Regulation 7 of the Road Traffic (NHS Charges)
Regulations 1999 and Regulation 5 of the Personal Injuries
(NHS Charges) (General) and Road Traffic (NHS Charges)
(Amendment) Regulations 2006
Injured person's representative details
Employment details
What to do now
Hospital details
All incidents on or after 29.01.07
Road Traffic Accidents only before 29.01.07