NEUROPATHY: How Pinprick Testing Can Help Detect Early Nerve Damage
1. NEUROPATHY
MAY/JUNE 2006 I DIABETIC MICROVASCULAR COMPLICATIONS TODAY I 31
L
eg ulceration — a serious com-
plication of diabetic peripheral
neuropathy (DPN) — frequently
leads to amputation. Several
widely recommended testing methods
are useful aids to predict DPN. Among
these methods, established convention
and clinical evidence maintain the
employment of large fiber modality test-
ing (eg, pressure/touch and vibration). It
might be speculated, however, that closer
scrutiny of the relevant neuropathophysi-
ology suggests that adequately executed
pinprick may still emerge as the superior
choice of testing modality.
The testing of cutaneous pinprick sen-
sibility is a routine medical procedure. It
has applications in family practice, dia-
betes, neurology, oncology, anesthesiology and in the ER.
Particularly, it has ramifications for the prognosis of condi-
tions associated with gross morbidity in which the patho-
physiology is dominated by small nerve fiber destruction.
The pinprick deficit produced by such small fiber popula-
tion loss is commonly reported to precede that of larger
fiber modalities including pressure/touch. It is hypothe-
sized, where appropriately discernible, that cutaneous pin-
prick sensibility may reflect the development of clinically
critical thresholds of neuropathy not revealed by testing
with other modalities.
PAIN AS A PROTECTIVE MECHANISM
It may be cliché — and possibly the more powerful for it
— that The Gift of Pain by Brand and Yancey is acclaimed as
a principal medium for establishing the value of pain to pro-
vide a protective mechanism against tissue damage.1
In con-
text, the Latin derivative, “nocere,” offers the translation2
“to
do harm.” Widely quoted and almost universally venerated,
the text’s standpoint on the critical role of nociception as a
defining element in the maintenance of health would be dif-
ficult to refute and is compatible with the definition offered
by the International Group For the Study of Pain, “An
unpleasant sensory and emotional experience associated
with actual or potential tissue damage, or described in
terms of such damage.”
It is reasonably assertable that the primary role of pain is
to caution the central nervous mechanism against somatic
insult. This is not a function generally attributed to either
pressure/touch or vibration, although that is not to say the
Cutaneous Pinprick
Sensibility as a
Screening Device
This method is overlooked, undervalued and critical in redefining
a clinically significant threshold for protective sensation.
BY BARRY L. JACOBS, DO
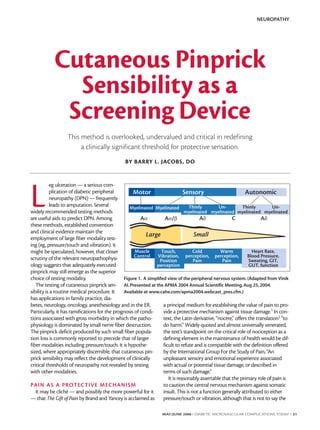
Motor
Large Small
Myelinated Myelinated
Aα Aα/β Aδ AδC
Thinly
myelinated
Muscle
Control
Touch,
Vibration,
Position
perception
Cold
perception,
Pain
Warm
perception,
Pain
Heart Rate,
Blood Pressure,
Sweating, GIT,
GUT, function
Un-
myelinated
Thinly
myelinated
Un-
myelinated
AutonomicSensory
Figure 1. A simplifed view of the peripheral nervous system.(Adapted from Vinik
AI.Presented at the APMA 2004 Annual Scientific Meeting,Aug 25,2004.
Available at www.cahe.com/apma2004.webcast_pres.cfm.)
2. events giving rise to tissue damage cannot overlap with
them. As an advanced warning device, however, pressure/
touch or vibration are not the primary physiological mecha-
nism. In the peripheral nervous system (Figure 1), withdrawal
of an extremity from noxious stimulation (damaging normal
tissue) is largely initiated by cutaneous nociceptors. The
central nervous system easily habituates to sustained neuro-
logical traffic, apart from that of pain. In contrast, sustained
exposure to a painful stimulus frequently generates an expo-
nential curve of sensitization.
Pain perception is a mechanism evolved to effect the
preservation of normal tissue integrity in which the diminu-
tion of performance must attract a concomitant potential
for reciprocal endangerment of the host tissue. One frustra-
tion for the examining practitioner is that a deficit of pain
perception may be a subtle but progressive affair that seems
beyond conventional primary methods of assessment.
According to Marks,3 some patients will have loss of normal
sensation as a result of nerve damage and hypofunction.
These patients will not be aware of disability until injury
and/or ulceration occur. This occult behavior gives rise to
the assertion that DPN, the most common peripheral neu-
ropathy in advanced nations,4,5 accounts for more hospital-
izations than all other diabetic complications combined. We
should appreciate that the potential for risk for damage
does not represent (nor require) absolute abolition of pain
perception rather than a reduction. Pain sensitivity can be
represented on a scale; increments of this scale should
roughly equate to a proportional risk of damage. Where
some degree of pain has occurred, deficit examination of
the affected tissues must be quantitative.
A CLINICALLY SIGNIFICANT THRESHOLD
FOR PROTECTIVE SENSATION
Almost without exception, studies employing a pinprick
as part of the DPN screening test criteria have imposed a
simple presence of perception test using sharpness rather
than degree. Variations of this technique have been
described, however, the general principle may take for
granted that a negative finding is revealed (1) by a failure to
discriminate between sharp and blunt or (2) to identify
sharp as compared with a predictably normal part of the
body (eg, shoulder). This does not accurately represent the
role of pinprick or the behavior of typical pathophysiologi-
cal degeneration.
The following is a common observation: Pain and tem-
perature perception are carried by and target nerve con-
stituents that are damaged principally and initially by meta-
bolic disorders including diabetes.6-11
It is well understood
that these are the small-fiber A delta and small-fiber C-pop-
ulation. The other tactile testing modalities (eg, touch/
monofilament and vibration) are carried out only by the
large fiber populations, which appear to deteriorate at a
later stage.
In tandem with its physiological function of providing
protection against tissue damage, there is a strong implica-
tion that pain deficit is a consequence of its early occur-
rence in the development of neuropathic ulceration com-
pared with the modalities carried by larger fibers. The
nature of DPN is progressive; the conventional notion of
protective sensation may lack sufficient discrimination for
refined diagnosis and prognostication. Findings from the
10,000-patient cohort North-West Diabetes Foot Care
Study12 provided significant support for this suggestion,
although even in this work, only crude pinprick technique
was employed, and focus was biased toward monofilament
assessment. An argument emerges for a method that
describes when a patient with diabetes has become vulner-
able to the effects of pain deficit. This approach requires a
refinement of the stages/thresholds at which loss of protec-
tive sensation become clinically significant. The refinement
would bolster the right of a normal distribution curve
where time runs along the x-axis.
LIMITATIONS TO QUANTIFICATION
WITH MONOFILAMENT
Testing pressure/touch is contentious; seeking to reveal
early pain deficit by focusing on large fiber testing modali-
ties would seem inconsistent with both the physiology and
the pathophysiology of the nerve constituent population.
Early loss of pressure/touch and the potential testing bene-
fits provided by detection would significantly be preceded
by deficit of pain or pinprick. Clinical information (derived
from modest diminution rather than complete absence of
cutaneous pinprick) would be extensive compared with the
degree of loss simultaneously demonstrable in large fibers
using pressure/touch.
The attractive aspect of assessment with the Semmes-
Weinstein monofilament is based on producing a degree of
objective quantification through the application of a repro-
ducible, calibrated stimulus. As is so frequently the case in
the minutiae of everyday practice, this method takes for
granted a number of assumptions. Aside from concern over
the lack of consistency between the available monofila-
ments (both commercially and offered by various pharma-
ceutical companies),13
it may be erroneous to assume that
the quantified stimulus of the test will be perceived as uni-
versal by the patient population. Tactile sensation is an espe-
cially idiosyncratic phenomenon that is a function of — and
perpetually influenced by — factors including manifesta-
tions of neurological arousal embracing any variant between
anxiety and relaxation (though it may also take into account
fatigue and ambient temperature). The same patient is likely
to provide two or three different responses to the same test
NEUROPATHY
32 I DIABETIC MICROVASCULAR COMPLICATIONS TODAY I MAY/JUNE 2006
3. NEUROPATHY
MAY/JUNE 2006 I DIABETIC MICROVASCULAR COMPLICATIONS TODAY I 33
over several occasions simply due to variation in personal
circumstance.
Between patients, and, for that matter, different practi-
tioners, the variance will be compounded making the
detection of subtle distinctions in sensitivity somewhat arbi-
trary. Where application of a more extreme stimulus is used
(eg, one in which the magnitude gravitates significantly to
the right of the normal distribution curve), the practitioner
is able to provide sufficiently gross stimulation to eclipse
subtle variations in circumstances and be more recognizable
as uniform between individuals or for the same individual
on different days.
The inability to perceive a 5.07-g monofilament repre-
sents a sensory threshold that is more than 50 times greater
than normal. This implies that approximately 98% of normal
sensory ability has been lost.14 The usefulness of extreme
stimulation for detecting subtle nerve damage, thus,
becomes questionable by virtue of the advanced deficit
required to fail to perceive it. The 10-g monofilament, there-
fore, is probably the least suitable instrument to detect early
deficit. It is perfectly adequate for consistently demonstrat-
ing unequivocal cases. The monofilament is established in
the literature as a reliable device for the prediction of neuro-
pathic ulceration. It must be recognized, however, that this
predictive value is compatible only with advanced stages of
degeneration. One disability score factor that particularly
betters monofilament testing is a preexisting history of
ulceration itself.12 So far, the value of the monofilament has
been only to signal advanced vulnerability.
PINPRICK AS A DESCRIBER OF CHANGE
The perceived presence/absence of a sharp stimulus as
an all or nothing criterion is insufficient to reveal early pain
deficit. In contrast, simple recognition of a reduction in pin-
prick sensibility, even when early, could be critical. A
redeeming feature of pinprick testing is not based on
objective quantifiability (although quantification is possible
with the use of adapted techniques),15
but the principle
that it can demonstrate deficit by comparison of a poten-
tially affected area to one that is expected to display an
acceptable degree of integrity elsewhere on the same sub-
ject. Findings are based upon the distinctions made by the
patient between these areas, thereby dispensing with the
need to compare to a predetermined marker.
Extraneous circumstances will be of little consequence;
they will be constant for the same patient, on the same day,
who is always compared to him or herself. All that is
required of the patient is to recognize a difference in acuity
of the pinprick stimulus. Visual analogue scales have shown
that patients are capable of demonstrating remarkable
consistency in identifying subtle distinctions in pain severi-
ty.16
By use of a simple comparison between affected and
normal areas of skin, patients are permitted to express even
the earliest and most subtle differences freely. Adaptations
to technique, such as those routinely employed by neurolo-
gists, can also be utilized to further refine this mode of
assessment for test sensitivity, accuracy and reproducibility.
As sensitive methods for monitoring progression of DPN
examination, procedures that exclude pinprick from the
tactile modalities are likely to be inadequate. It is unsurpris-
ing that even in the current popular climate, pinprick is reg-
ularly recommended as a best practice for screening.17-22 It
is suggested that this method remains largely neglected by
the health care provider community. There seems satisfac-
tory evidence to effect a more reflective and potentially
effective approach simply by drawing upon the resources
of evidence-based physiology and revisiting with a more
objective viewpoint some of the existing literature. ■
Barry L. Jacobs, DO, is in the Visiting Lecturer
Department of Rehabilitation Medicine at
Manchester Royal Infirmary, in Manchester, UK.
He may be reached at clinical@medipin.net or
+44 0 780 1986 515.
1. Brand P, Yancey P. The Gift of Pain. Zondervan. Reprint edition (September 1, 1997).
2.OxfordEnglishDictionary,2ndEd.OxfordUniversityPress.1991;5:454.
3.MarksJB.Theforgottencomplication.ClinicalDiabetes.2005;23:3-4.
4.VinikAI,ParkTS,StansberryKB,etal.Diabeticneuropathies.Diabetologia.2000;43:957-973.
5.VinikAI.Neuropathy:newconceptsinevaluationandtreatment.SouthMedJ.2002;95(1):21-23.
6.Brown.NaturalprogressionofdiabeticneuropathyintheZenarestatStudypopulation.DiabetesCare.
2004;27:1153-1159.
7.SosenkoJM,KatoM,SotoRA,etal.Specificassessmentofwarmandcoldsensitivitiesinadultdia-
beticpatients.DiabetesCare.1988;11:481-483.
8.ZieglerD,MayerP,GriesFA. Evaluationofthermal,pain,andvibrationsensationthresholdsinnewly
diagnosedtype1diabeticpatients.JNeurolNeurosurgPsychiatry.1988;51:1420-1424.
9.GuyRJC,ClarkCA,MalcolmPN,WatkinsPJ.Evaluationofthermalandvibrationsensationindia-
beticneuropathy.Diabetologia.1985;28:131-137.
10.HendriksenPH,OeyPL,WienekeGH,etal.Subclinicaldiabeticpolyneuropathy;earlydetectionof
involvementofdifferentnervefibretypes.JNeurolNeurosurgPsychiatry.1993;56:509-514.
11.SaidG,SlamaG,SelvaJ.Progressivecentripetaldegenerationofaxonsinsmallfibrediabetic
polyneuropathy.Brain.1983;106:791-807.
12.AbbottCA,CarringtonAL,AsheH,fortheNorth-WestDiabetesFootCareStudy.TheNorth-West
diabetesfootcarestudy:incidenceof,andriskfactorsfor,newdiabeticfootulcerationinacommunity-
basedpatientcohort.DiabetMed.2002;19:377-384.
13.LaveryL.Screeingfordiabeticneuropathy.Presentedatthe2004AmericanPodiatricMedical
AssociationAnnualScientificMeeting.August22-25,2004.Boston.
14.JengC,MichelsonJ,MizelM.Sensorythresholdsofnormalhumanfeet.FootAnkleInt.
2000;21:501-504.
15.YoungMJ,BoultonAGM,MacleudAF,etal.Multicenterstudyoftheprevalenceofdiabeticperiph-
eralneuropathyintheUK.Hospitalclinicpopulation.Diabetologia.1993;150-154.
16.KellyAM.Theminimumclinicallysignificantdifferenceinvisualanaloguescalepainscoredoesnot
differwithseverityofpain.EmergMedJ.2001;18:205-207.
17.Diabetes(2001)MedicalPracticeGuidelines.StateofFlorida,AgencyForHealthCare
Administration.Availableathttp://www.fdhc.state.fl.us/diabetes/notice.shtml.AccessedApril24,2006.
18.BoultonAJ,VinikAI,ArezzoJC,etal.Diabeticneuropathies:AstatementbytheAmericanDiabetes
Association.DiabetesCare.2005;28:956-962.
19.BoultonAJ,MalikRA,ArezzoJC,SosenkoJM.Diabeticsomaticneuropathies.DiabetesCare.
2004;27:1458-1486.
20.BrownMJ,BirdSJ,WatlingS,etal.NaturalprogressionofdiabeticneuropathyintheZenarestat
Studypopulation.DiabetesCare.2004;27:1153-1159.
21.PerkinsB,ZinmanB,OlaleyeD,BrilV.Simplescreeningtestsforperipheralneuropathyinthedia-
betesclinic.DiabetesCare.2001;24:250-256.
22.JacobsB,LewisD.Valueofpinprickinfindingperipheralneuropathyindiabetesmellituspatients.
PresentedattheWorldFamilyDoctorAssociation,WONCAEuropeRegionalConference.June18-21,
2003.Ljubljana,Slovenia.
4. NEUROPATHY
JULY/AUGUST 2006 I DIABETIC MICROVASCULAR COMPLICATIONS TODAY I 33
C
utaneous pinprick sensibility testing is rou-
tinely used in neurology and diabetes. It is
asserted here that the test is valuable for the
prognoses of conditions with pathophysiolo-
gies dominated by small nerve fiber destruction.
Contemporary literature neglects neurological pin-
prick among the cutaneous modalities. Rarely is it clin-
ically or technically reviewed for its diagnostic virtues,
however, closer scrutiny of the relevant neuropatho-
physiology suggests that adequately executed pinprick
is a logical choice.
The pinprick deficit produced by small fiber popula-
tion loss is commonly reported to precede that of
light touch. It may reflect the development of clinically
critical thresholds of neuropathy not revealed by test-
ing with other modalities. The following represents
part of a larger peer-reviewed effort to address issues
of clinical efficacy and infection control.
Nerve constituents typically damaged by metabolic
disorders (eg, diabetes) are small fiber populations,
implying that protective sensation (ie, focusing on
larger-diameter fiber populations), as opposed to pro-
tective pain may lack sufficient discrimination for
refined diagnosis and prognostication.1-6
Pinprick data
from the 10,000-patient cohort North-West Diabetes
Foot Care Study corroborates this notion.7
Where early
detection of neuropathic change is considered useful,
there emerges a case to redefine the stages or thresh-
olds at which loss of protective sensation is clinically
apparent.
Early diagnosis of diabetic peripheral neuropathy
(DPN) is a critical part of clinical management.
Combined with proper management, it may avoid
debilitating diabetes complications. Yet, recent
Diabetes UK research showed that people may have
diabetes for 9 to12 years before they are diagnosed.8
By this stage, many patients may develop neuropathy,
and their responses to standard examination proce-
dures are likely to demonstrate altered nerve function.
Techniques to identify DPN risk factors are usually
applied at annual check-ups, although it is contended
that current techniques are crude and may be insuffi-
ciently sensitive to detect the early deficit. If so, we
may fail to predict subtle loss of protective thresholds
in time to avoid critical management of complications.
MISCONCEPTIONS ABOUT
CUTANEOUS PINPRICK MODALITY
An evidence-based approach supplies us with a reli-
able application in the clinical setting. Ascertaining
and generating a reliable basis for description and
reproduction of test conditions may eclipse estab-
lished understanding, not through contradiction but
rather by distraction. Some human physiology aspects
cannot be quantified though preconceived models of
function.
Small nerve fiber destruction is largely progressive,
and therefore the deficit endured is incremental. In
Cutaneous Pinprick
Sensibility as a
Screening Device
Part Two: Enhanced diagnosis of diabetic peripheral neuropathy using
refined technique and dedicated single-use precision technology.
BY BARRY L. JACOBS, DO
Recent Diabetes UK research
has shown that people may have
diabetes for 9 to 12 years before they
are diagnosed.
5. order to accurately reflect typical pathophysiological
function, pinprick sensitivity deficit should be discern-
able on an analog scale. Pain perception is a subjective
affair and may vary (1) among the patient population
and (2) in the same patient under differing conditions
(eg, environment and emotion). Pain sensitivity is in a
state of perpetual flux. We need an objective scale,
intended to quantify pinprick deficit by comparison
with a standard measure almost physiologically impos-
sible except on the grossest crude scale (ie, the most
common scale used in pinprick assessment). A stan-
dard measure simply does not exist. Typically, a binary
or digital on-or-off approach is employed to test the
patient’s ability to (1) make the distinction between
sharp and blunt stimuli or (2) simply recognize the
presence of a painful one. This technique imposes a
model of neuropathophysiological behavior that is
incompatible with human function. The clinical obli-
gation is not to demonstrate the absence of pain per-
ception, but to reveal its early diminution. The
employment of appropriate technique is key.
STANDARDIZING IDIOSYNCRATIC
SENSITIVITY
A refined pinprick test should enhance the diagnos-
tic implications of the neuropathic state. Because
cutaneous sensitivity varies among the normal popula-
tion, the notion of a standardized threshold of normal
perception is somewhat academic. Nonetheless,
patients can reliably express subtle pain manifesta-
tions.9
The aim of pinprick testing, in the first instance,
is to detect subtle changes in deficit rather than com-
plete obliteration. A more practical approach revolves
around the old-fashioned but still-valid technique of
comparison. As with the testing of motor power and
reflexes, the practitioner can demonstrate even subtle
clinical deficit by juxtaposing one aspect of the physi-
ology to a comparable region. The objective is to
demonstrate the presence of clinical deficit by com-
paring a potentially affected area to one that displays
an acceptable degree of integrity. The practitioner
nominates a control area (eg, proximal part of a limb
or the trunk) to establish an adequate example of nor-
mal sensitivity by evoking an average response to stim-
ulation.
REPRODUCIBILITY IN TESTING –
THE ‘AVERAGE’ RESPONSE
One of the major flaws in any clinical diagnosis is
test consistency. Cutaneous pinprick assessment is par-
ticularly vulnerable to the variables that promote test
inconsistency. Among these is the random distribution
of nociceptors in the skin, strength of stimulation used
per application, and sensitization to the stimulus
depending on the period for which the stimulation is
maintained. There is a simple solution for reducing
this natural standard deviation: make multiple applica-
tions over a predetermined area such as the periphery
or a dermatome.10 Repetitious applications level stim-
ulation to an average where minor variations in appli-
cation pressure and contact location become statisti-
cally diminished. This technique is simple to perform
and rapid — taking perhaps seconds at a time.
Immediately, the practitioner has established an ade-
quate example of normal sensitivity in the nominated
control region. The test area should be addressed.
Continuous comparison between the two territories is
established by asking the patient to make distinctions
between them. This permits the expression of early
subtle, though potentially critical, distinctions in sensi-
tivity and is described as the Continuous Pinprick
Comparison Method (CPC). The technique can pre-
cisely gauge an area of deficit and plot progression of
the condition, possibly in response to management,
simply by mapping out subtle loss rather than by
determining absence of pain perception.
CRUDE PINKPICK STIMULUS
Pinprick stimulation is a manifestation of skin
stretch rather than sharpness and is difficult to test
adequately. Ironically, the sharper the point, the less
the skin is disturbed in a fashion that activates cuta-
neous mechanoreception (Ruffini/SAII afferents) to
report nociception. In patients with diabetes, sensitivi-
ty loss often develops in tandem with skin weakness
and, when a crude pinprick test is employed, touch
modality alone is stimulated so that excessive pressure
is required to achieve a pinprick stimulus. This may
lead to skin penetration and reveals only extreme sen-
sory loss. A more sensitive technique to measure
deficit dictates that these patients require consistent
augmentation of pinprick acuity in the absence of
excessive application pressure while simultaneously
promoting test application reproducibility. Conditions
dictating optimum performance for pinprick include
NEUROPATHY
34 I DIABETIC MICROVASCULAR COMPLICATIONS TODAY I JULY/AUGUST 2006
A refined pinpick test should enhance
the diagnostic implications of the
neuropathic state.
6. NEUROPATHY
JULY/AUGUST 2006 I DIABETIC MICROVASCULAR COMPLICATIONS TODAY I 35
innovation of a dedicated instrument intended to
achieve best practice and is still compatible with the
everyday clinical setting. In summary, the aims of this
program for enhanced cutaneous pinprick test were
expressed by:
• Rapid application in the primary care setting;
• Refined diagnosis of significant deficit through the
achievement of neurophysiologically enhanced pin-
prick stimulus;
• Earlier definition and diagnosis of clinically signifi-
cant thresholds at reduced application pressures;
• Examination to include A-delta and C-nerve fiber
constituents;
• Promotion of test reproducibility with more reli-
able monitoring of neuropathic progression; and
• Improvement of infection control issues.
This program motivated the development of a sin-
gle-use precision technology designed to enhance the
clinical sensitivity of cutaneous pinprick testing. It is
proposed that this has been achieved by manipulating
multiple factors that influence acuity perception and
consistency. The resulting device is an 80-mm dispos-
able instrument that can be injection-molded for mul-
tiple production and described for the purposes of the
US Food Drug Administration as the Single-Use
Protected Neurological Pin. For more public dissemi-
nation, it has been named Medipin (Figure 1) (in the
United States, marketed by US Neurologicals, Kirkland,
Wash, in the United Kingdom, Mastermedica Limited,
Worcestershire, UK).
The active element of this instrument consists of a
short faceted point — acutely delineated by its sur-
faces and edges and inclined to stretch rather than
penetrate the skin surface — within an annular appa-
ratus that encircles the point with a perimeter of dull
stimulation. By stretching the skin and contrasting the
sharp stimulus of this highly demarcated point with
that of the annulus, it is possible to emphasize the
neurological phenomenon of lateral inhibition where
functional connections, formed in the central nervous
system, highlight differences between areas of sensa-
tion.11 At each application, the device generates a
focused and well-defined center-surround field effect,
comparable with that occurring in visual phenomena.
This effect augments the acuity of pinprick
stimulation12,13 and is an innovation intended to
achieve C-nerve fiber stimulation, although this has yet
to be verified.
Anecdotally, patients report a frequent pattern of
stimulation consisting of an initial sharp stimulation
followed by a deeper more persistent sensation.
Current understanding of nociceptor behavior is con-
sistent with this representing A-delta and C-nerve fiber
responses respectively, though further study is needed.
The combination of acuity and reproducibility is
intended to enhance test sensitivity. This high sensitivi-
ty also suggests that less application pressure is
required to generate adequate stimulation versus
other methodologies. Limitation to point penetration,
imposed by seating it within the annular structure, is
intended to render cross infection from accidental lib-
eration of bodily fluids. The annulus also serves to
shield the practitioner from the point during applica-
tion and offers more protection against accidental
needle-stick injury. The annulus design serves to pro-
mote test consistency through standardizing point
penetration as well as infection control.
A similar solution for standardizing point penetra-
tion was discovered in the immunology field. A com-
parable design was developed to produce consistent
pinpricks to penetrate the skin surface and investigate
allergy. In this design, a narrower point achieves pene-
tration of the skin, whereas the Medipin adopts a
wider point base and a more favorable point height to
annular radius ratio to prevent it.14-16
Despite these
precautions, skin penetration should never be regard-
ed with complacency, and disposal remains key to
appropriate infection control.
PRACTICAL APPLICATION
Observations were drawn from routine practice and
modifications were made during its development. A
textured shaft to facilitate handling was incorporated.
Surgeons felt that consistency was a matter of light grip
and minimal skin contact so that axial slippage was pos-
sible during its application. A later innovation was the
snap-off tab, designed to protect the point prior to
Figure 1. The Medipin is an 80-mm disposable instrument.
7. application and negate restoration of the device after-
wards, dissuades inexperienced clinicians from attempt-
ing to reuse a disposable device on multiple occasions.
With this last view in mind and the perpetual possi-
bility of micropenetration, European practitioners
addressed the frequent lack of sharps disposal contain-
ers. They destroyed the device’s point by compressing
it against a hardened usually metallic, surface. The
point was designed to collapse without breaking off
from the main body of the instrument and can there-
fore be rendered reasonably safe. In the United States,
this design is less advantageous because sharps dispos-
al facilities are not a common issue, however, it
remained an advantage over metal-based devices
where the clinician might not have a choice.
The device has been assessed, somewhat informally,
at several reputable institutions worldwide, and it is
currently engaged in clinical studies. It has also been
used quite extensively in the primary care setting. In all
cases, consultation guided application and was sup-
ported by specific directions:
1. Break tab to expose point, avoiding contact with
fingers.
2. Grasp device between thumb and index finger
lightly enough to permit slight axial slippage.
3. Apply to the skin surface at a perpendicular angle,
making several quick applications around the same
locality. Repeated application diminishes standard
deviation error and promotes average stimulation.
Press firmly but carefully, using controlled, repetitive,
percussive contact. Avoid high amplitude or stabbing
actions as skin penetration should never be regarded
as impossible.
4. To prevent reuse, destroy point by compressing
against a hard surface and/or dispose of in a biohazard
container.
RESULTS
Initial impressions from health care professionals
diagnosing and treating peripheral neuropathy have
been favorable. Patients with diabetes tolerated the
device and technique very well, and nurses found the
technique easy to learn. Demonstration of sensory
deficit appears reliable between practitioners, and fur-
ther study is indicated on this approach.17,18
The pertinent pathophysiology strongly suggests
that cutaneous pinprick testing should be the primary
choice of modality. Although frequently misunder-
stood or neglected, an appropriate clinical approach
that offers clinicians access to enhanced efficacy in the
early diagnosis of diabetic peripheral neuropathy is
easily achieved. In combining an easy-to-apply, single-
use technology with physiologically corroborated, evi-
dence-based technique, we move toward the promo-
tion of test standardization and accuracy of routine
pinprick testing and simultaneously reducing fear of
cross or self-infection. ■
Barry L. Jacobs, DO, is in the Visiting Lecturer
Department of Rehabilitation Medicine at
Manchester Royal Infirmary, in Manchester, UK.
He may be reached at clinical@medipin.net or
+44 0 780 1986 515.
1. MJ Brown, Bird SJ, Watling S, et al. Natural progression of diabetic neuropathy in the
Zenarestat Study population. Diabetes Care. 2004;27:1153-1159.
2. Sosenko JM, Kato M, Soto RA, et al. Specific assessment of warm and cold sensitivities in
adult diabetic patients. Diabetes Care. 1988;11:481-483.
3. Ziegler D, Mayer P, Gries FA. Evaluation of thermal, pain, and vibration sensation thresholds
in newly diagnosed type 1 diabetic patients. J Neurol Neurosurg Psychiatry. 1988;51:1420-
1424.
4. Guy RJC, Clark CA, Malcolm PN, Watkins PJ. Evaluation of thermal and vibration sensation
in diabetic neuropathy. Diabetologia. 1985;28:131-137.
5. Hendriksen PH, Oey PL, Wieneke GH, et al. Subclinical diabetic polyneuropathy; early detec-
tion of involvement of different nerve fibre types. J Neurol Neurosurg Psychiatry. 1993;56:509-
514.
6. Said G, Slama G, Selva J. Progressive centripetal degeneration of axons in small fibre dia-
betic polyneuropathy. Brain. 1983;106:791-807.
7. Abbott CA, Carrington AL, Ashe H, et al The North-West Diabetes Foot Care Study: incidence
of, and risk factors for, new diabetic foot ulceration in a community-based patient cohort.
Diabet Med. 2002;19:377-384.
8. Diabetes UK. Position Statement: Early diagnosis of patient with type 2 diabetes, 2006.
Available at www.diabetes.org.uk/infocentre/state/downloads/earlyid.doc.
9. Price DD, Bush FM, Long S, Harkins SW. A comparison of pain measurement characteristics
of mechanical visual analogue and simple numerical rating scales. Pain. 1994;56:217-226.
10. Frisso A, Potts, MD. Peripheral Neuropathy. Merck Medicus, Best Practice of Medicine;
2001 April; merck.micromedex.com/index.asp?page=bpm_brief&article_id=BPM01NE12.
11. Department of Physiology, Berkeley University, Ca, USA. Lateral Inhibition. Available at
www.totoro.berkeley.edu/teaching/AA_teaching_aids.html.
12. Robert M. Berne. Principles of Physiology. (Philadelphia, Mosby). 2001. Chpts. 6 - 9, 12-
14.
13. Ebner FF, Armstrong-James MA. Intracortical processes regulating the integration of sen-
sory information. Prog Brain Res. 1990;86:129-141.
14. Perrin LF, Dechamp C, Deviller P, Joly P. Reproducibility of skin tests. A comparative study
of the Pepys prick test and the Morrow-Brown needle and their correlation with the serum IgE
level. Clinical Allergy. 1984;14:581-588.
15. Adinoff AD, Rosloniec DM, McCall LL, Nelson HS. A comparison of six epicutaneous
devices in the performance of immediate hypersensitivity skin testing. J Allergy Clin Immunol.
1989; 84:168-174.
16. Demoly P, Bousquet J, Manderscheid JC, et al. Precision of skin prick and puncture tests
with nine methods, J Allergy Clin Immunol. 1991;88:758-762.
17. Jacobs B, Lewis D. Value of pinprick in finding peripheral neuropathy in diabetes mellitus
patients. Poster presented at the World Family Doctor Association, WONCA Europe Regional
Conference. June 18-21, 2003. Ljubljana, Slovenia.
18. Jacobs B, Lewis D. Refined diagnosis of diabetic peripheral neuropathy with enhanced pin-
prick perception using novel single-use precision instrument design and technique.
Abstract/poster presentation at Global Diabetic Foot Conference 2006. March 23-25. Los
Angeles.
NEUROPATHY
36 I DIABETIC MICROVASCULAR COMPLICATIONS TODAY I JULY/AUGUST 2006
Would you like to comment on article? Do
you have an article topic to suggest? Do you
wish to tell us how valuable DMCTODAY is to
your practice? We would love to hear from you.
Please e-mail ckoury@bmctoday.com regarding
this publication.
SHARE YOUR FEEDBACK