1. METHODS
Patients diagnosed with Orofacial pain conditions from multidisciplinary pain clinics within the
Oral Surgery Department of the King’s College Hospital Dental institute were included.
Each patient was required to complete a previously validated clinical questionnaire. (Please
see the handouts)
PAIN CONDITIONS CASES
(%)
PERSISTENT IDIOPATHIC 198 (59.1)
NEURALGIA 51 (15.2)
NEUROVASCULAR 8 (2.4)
INFLAMMATORY 15 (4.5)
PERSISTENT IDIOPATHIC + INFLAMMATORY 6 (1.8)
PERSISTENT IDIOPATHIC + NEUROVASCULAR 3 (0.9)
PERSISTENT IDIOPATHIC + NEURALGIC 3 (0.9)
NEURALGIC + INFLAMMATORY 3 (0.9)
NEURALGIC + NEUROVASCULAR 1 (0.3)
NOT AVAILABLE 47 (14)
TOTAL 335 (100)
Table 1: General Demographics of patients
2
TOTAL CASES 335
FEMALE:MALE 234:84
AGE RANGES 11 TO 89 YEARS
MEAN AGE (YEARS) 44.62 (SE=0.85)
The Orofacial pain conditions were then
classified based on Woda et al. (2005)
classification.
Data was analysed using MS Excel and IBM
SPSS 19.
The statistical tests used included f-test, t-test
and Anova test.
P<0.05 indicated statistical significance.
ANALYSIS
PARTICIPANTS
CLASSIFICATION
ASSESSMENT
THE INFLUENCE OF PSYCHOLOGICAL, BEHAVIOURAL AND SOCIAL FACTORS
ON PAIN EXPERIENCE IN PATIENTS WITH CHRONIC OROFACIAL PAIN
STUDENT: ARTI MEENAKSHI SRINIVASAN SUPERVISORS: DR. ZEHRA YILMAZ, PROF TARA RENTON
Assessment of pain was carried out using
- Brief Pain Index, which consist of
visual analog scale ranging from 0 to 10,
where 0= no pain, 10= worst possible
pain imaginable.
Assessment of anxiety and depression
was carried out using
- Hospital Anxiety and Depression Scale,
a self reported questionnaire with 14
multiple choice questions each scored
from 0 to 3.
The factors considered included
- Level of information the patient has
about their pain condition
- Eight different personal resources (i.e.
functionality)
- Level of education
- Marital status
- Living conditions
- Age group Table 2: Classification of patients
REFERENCES
1. Edited by H. Merskey and N. Bogduk (1994) Classification of Chronic Pain, Second Edition,
IASP (pp 209-214).
2. Renton, T., Durham, J., 7 Aggarwal, V. R. Expert Review neurotherapeutics 12(5), 569-76.
3. Yazdi, M., Yilmaz, Z., Renton, T., & Page, L. (2012). Oral Surgery, 5(4), 173–181.
INTRODUCTION
AIM
Pain is defined as being “ an unpleasant sensory and emotional experience
associated with actual or potential tissue damage or described in terms of such
1
damage”.
2
Orofacial pain affects approximately 7% of the UK population.
The trigeminal nerve and the facial nerve are the major sensory networks associated
2
with pain perception in the orofacial regions.
Chronic orofacial pain (COFP) cause psychological distress, involve psychogenic
3
intensification or in itself be a pure psychogenic pain altering pain experience.
To investigate the effect of different behavioural and social factors on the level of
pain, anxiety and depression experienced by patients with COFP conditions.
Patients with inadequate level of information and poor personal resources would
show increased pain experience, anxiety and depression.
Those with neuralgic pain would show worse experience when compared to those
with idiopathic persistent pain.
Poor social environment can negatively affect pain experience resulting in
interference with daily activities.
HYPOTHESES
CONCLUSIONS
Psychosocial and behavioural factors have a debilitating effect on patients with COPD amongst whom, patients with idiopathic persistent pain
are likely to present with more severe psychological morbidity.
Age, sex, marital status, level of information and education, and functionality play a key role by affecting the patients' pain experience and mood.
All these social factors should also be considered, examined and monitored while treating patients with Chronic Orofacial pain.
DISCUSSION AND FUTURE WORK
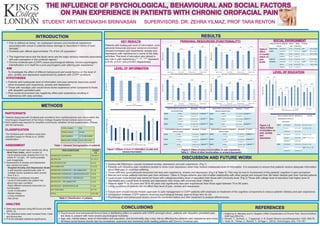
RESULTS
LEVEL OF INFORMATION
KEY RESULTS
LEVEL OF EDUCATION
SOCIAL ENVIRONMENTPERSONAL RESOURCES (FUNCTIONALITY)
Patients with inadequate level of information, poor
personal resources and poor social environment
showed increased pain experience, anxiety and
depression with interference in some of the daily
activities. The level of education also played a
key role in pain experience.(**, ***, **** represent
p<0.05, p<0.01 and p<0.001 respectively)
Figure 1:Effects of level of information on pain and
anxiety/depression.
Figure 2: Effect of some functionalities on pain experience.
Table 3 : Effect of other functionalites on anxiety/depression
Table 4
Effect
of marital
status on
pain
levels
Figure 3 &
Table 5:Effect
of education on
pain, anxiety
and
depression
Inadequate information causes increased anxiety, depression and pain experience. (Fig 1)
Patients with idiopathic pain conditions tended to show more depression when they receive inadequate level of information. It is necessary to ensure that patients receive adequate information
about their pain to minimise suffering.
Those with very good personal resources had less pain experience, anxiety and depression (Fig 2 & Table 3). This may be due to involvement of the patients' cognition in pain perception.
Married and single patients had less pain than widowed. (Table 4) Single patients also had a better relationship with other people and enjoyed their life better despite pain than married patients.
Level of pain experienced was worse for those with college/secondary level of education than those with University level. (Fig 3) Those with college level of education had higher level of
depression and overall level of anxiety and depression than those with university level. (Table 5)
Patients aged 11 to 29 years and 30 to 49 years had significantly less pain experiences than those aged between 70 to 89 years.
Living conditions of patients did not affect their level of pain, anxiety and depression.
Future work should include Holistic approach to pain management in COFP patients with emphasis on treatment of the cognitive components to reduce patients’ distress and pain experience.
Comparison between COFP patients receiving psychological therapy against those who do not.
Psychological and behavioural factors should be monitored before and after treatment to analyse effectiveness..