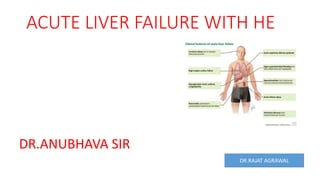
This document describes the case of a 9-year-old male child presenting with acute liver failure. On examination, the child was deeply jaundiced, had hepatomegaly with ascites, and decreased mental status. Laboratory tests showed coagulopathy and hyperbilirubinemia. Leptospirosis testing was positive. New guidelines from NASPGHAN and ESPGHAN in 2022 update fluid management and glucose monitoring recommendations compared to the 2017 guidelines. Key criteria for liver transplantation including King's College criteria and factors prognostic of poor outcome are also discussed.
2. CASE PRESENTATION OF ACUTE LIVER FAILURE
9YRS OLD MALE CHILD PRESENTED IN ER WITH CHIEF COMPLAINT OF FEVER SINCE 15
DAYS,YELLOWISH DISCOLOURATION OF SKIN SINCE 5DAYS ,UNRESPONSIVE SINCE DAYS OF
ADMISSION.
ON EXAMINATION :CHILD WAS SICK
DEEPLY ICTERIC
PALLOR +
RESPIRATORY EXAMINATION : CHEST B/L CLEAR
ABDOMINAL EXAMINATION :S/O HEPATOMEGALY WITH ASCITES
NEUROLOGICAL EXAMINATION : S/O GCS SCORE E2V1M4
NO MENINGEAL SIGN
DTR BRISK
HYPOGLYCEMIA RBS 50 MG/DL
SKIN EXAMINATION :PURPURIC RASHES +NT AND BLEEDING POINT AT THE SITE OF
ELECTRODE
3. CHILD WAS ELECTIVE INTUBATION BECAUSE GCS <8
INVESTIGATION 1. COAGULATION PROFILE IS
DEARRANGEDS PT >120 SEC WITH INR NOT RECORDABLE
2. TOTAL BILIRUBION 18.13 MG/DL
FUNDSUS EXAMINATION NORMAL
OPTIC DISC DIAMETER ALSO NORMAL
SERUM SODIUM 126 MG/DL
LEPTOSPIROSIS IGM +VE
5. he diagnosis and
management of
PALF were
released by the
North American
Society for
Pediatric
Gastroenterology
, Hepatology, and
Nutrition
(NASPGHAN) and
the Euro-pean
Society for
Pediatric
Gastroenterology
, Hepatology, and
Nutrition
(ESPGHAN)
6. NEW GUIDELINES FROM NASPAGHAN AND ESPHAGAN (2022)
COMPARE WITH 2017 GUIDELINES
2022 2017
1.FLUID AND ELECTROLYTE –IVF 90% TOTAL MAINTAINCE FLUID
INITIAL FLUID –N/2 NS WITH 10% DEXROSE
WITH 15 meq/l K+ve(RL AVOID)
GLUCOSE TARGET SATURATION 90-120 MG/DL
SERUM NA+145-155 meq/dl
7.
8. N-acetylcysteine This agent is a specific antidote
in cases of FHF due to an overdose of
paracetamol (acetaminophen). It probably works
by replenishing glutathione stores and preventing
free radical damage.8 It is useful if started within
10e16 h along with other supportive measures.
The regimen consists of giving 140 mg/kg orally
followed by 70 mg/kg every 4 h for 17 doses
spread over 72 h or until the serum paracetamol
concentration falls to zero. At this dose, it is
remarkably free of toxicity.61
10. Parameter
Points assigned
1 2 3
Ascites Absent Slight Moderate
Bilirubin
<2 mg/dL (<34.2
micromol/L)
2 to 3 mg/dL (34.2 to
51.3 micromol/L)
>3 mg/dL (>51.3
micromol/L)
Albumin >3.5 g/dL (35 g/L)
2.8 to 3.5 g/dL (28 to
35 g/L)
<2.8 g/dL (<28 g/L)
Prothrombin time
(seconds over control)
or
<4 4 to 6 >6
INR <1.7 1.7 to 2.3 >2.3
Encephalopathy None Grade 1 to 2 Grade 3 to 4
Child-Pugh classification of severity of cirrhosis
11. Arterial pH < 7.30
INR > 6.5 (PT > 100 sec)
Creatinine > 3.4 mg/dL (300 µmol/L)
Grade III or IV hepatic encephalopathy
• Grade – III hepatic encephalopathy – Marked confusion, incoherent speech, sleeping most of the time
but arousable to vocal stimuli
• Grade – IV hepatic encephalopathy – Comatose, unresponsive to pain; decorticate or decerebrate
posturing
Lactate > 3.5 mmol/L after fluid resuscitation (<4 hrs) OR lactate > 3 mmol/L after full fluid resuscitation
(12 hours)
Phosphate > 3.75 mg/dL (1.2 mmol/L) at 48-96 hours
:
The presence of one of the following should prompt a
referral/transfer to a liver transplantation center
King college criteria for liver
transplantation