
Recommended
More Related Content
What's hot
What's hot (20)
Similar to ECT Presentation.ppt
Similar to ECT Presentation.ppt (20)
Recently uploaded
Recently uploaded (20)
ECT Presentation.ppt
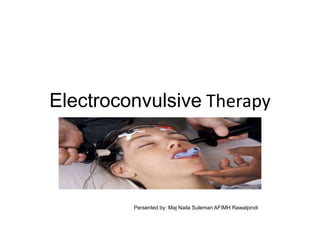
- 1. Electroconvulsive Therapy Review the outline in notes Persented by: Maj Naila Suleman AFIMH Rawalpindi
- 2. Learning Objectives • Identify Diagnosis for ECT • Identify Equipment Needed • Explain Electrode Placement • Seizure Duration • Explain Mini Mental Exam • Identify post Procedure Monitoring • Describe Discharge Requirement • Contraindications • Common ECT Side Effects • Medications Contraindicated for ECT
- 3. Definition of ECT • ECT is a method where electric currents are passed through the brain, deliberately triggering a momentary seizure. Through this electrical stimulation of the brain, ECT appears to produce alteractions in brain chemistry that can enable a rapid reduction in the signs and indicators of selected psychiatric and mental health disorders, e.g., severe depression and bipolar diseases.
- 4. Mechanism of Action • The mechanism of action is unknown • Research determined that ECT increase monoamine transmitters (Dopamine & Serotonine) • ECT Increase the release of Central neuro peptide, the neuro endocrine hypothesis suggest insufficiency of the hypothalamic mood maintaining peptide • MRI revealed reduction in global connectivity Ultimately, our brain and CNS is so complex there is no clear, definitive answer on exactly how ECT works
- 5. Indications for ECT Patients who are resistant to pharmacological interventions and present with: • Major Depressive Disorder (MDD) • Bipolar Disorder • Schizophrenia • Parkinsonism, not responding to Medication
- 6. Equipment /Supplies • Nurses responsibility is to ensure availability of: • ECT Machine • Electrodes • Gel • Cardiac Monitor • Bite Block • Blood Pressure Machine • Suction Machine
- 7. Mini Mental Exam • The MMSE is a reliable tool that takes 5 minutes to complete the focus on Appearance Behavior Thought Process
- 8. Stages of Nursing Process • ECT patient sequence process – Pre Procedure Area – Treatment Room – Recovery Room – Phase II
- 9. Pre-Procedure • Pre- Op Nurses completes the pre- ECT checklist Consisting of • Verification of NPO status • Removal of Jewelry clothing etc. • Verifying Allergies • Verifying patient awareness of the procedure • Obtain baseline Vital signs • Verifying Medical clearance • Existence of Medical results • Verify existence signed consents • Obtain Intravenous access
- 10. ECT Procedure • Anesthesia is administered • Electrodes place either unilaterally, bilaterally and bifrontal • The electrical impulse of 70 – 150 V • The desired seizure duration of 15 – 50 seconds • Chemical changes occur
- 11. Phase I/ Recovery Nurse Responsibility • The patient is assessed and monitored according to best practice standards and facility guidelines as Follows: » Provide continuous cardiac monitoring » Blood pressure every 15 minutes or less » Continuous Pulse Oximetry » Assess LOC / Mini Mental Exam Discharge Criteria Blood pressure within 20% of baseline Room air saturation at baseline Follow commands No Post Op nausea/ headache Oriented to person place & time
- 12. Phase II / Recovery • Once discharge criteria is met the patient then transitions to the next level of care • Inpatient room • Outpatient – Home with responsible adult D/C Criteria Includes: Oriented x 3 Tolerating food and drink No nausea, headache
- 13. Side Effects / Adverse Reactions • Memory loss – anterograde and retrograde • Nausea • Headache • Muscle aches • Tardive seizure – rare potentially fatal • Considered safe for children, pregnant women and elderly ECT current death rate is approximately 2 per 100000 treatments
- 14. Condition with increased Risk/ Contraindications • Vascular aneurysms • Central nervous system conditions associated with intracranial pressure • Some brain tumors • Recent cerebral infarct • Severe pulmonary or other organ system disease presenting anesthesia risk No true contraindications for ECT
- 15. Medication Contraindications • Avticonvulsants • Interfere with seizure production • Antieleptic mood stabilizers • Tapered and stopped before ECT • Benzodiazepines • Potential anticonvulsant • Lithium • Neuro toxicity & poor outcome
- 16. Conclusion • ECT is a safe treatment for patients who are resistant to other forms of therapy • The continued success of ECT patients outcomes are dependent on the ECT team especially the nurses who care for the patients and are knowledgeable in their assessment and care pre and post procedure. Prepared by: Maj Naila Suleman AFIMH Rawalpindi
Editor's Notes
- I. Introduction A. Standard Vb of the ANA Standards of Psychiatric-Mental Health Nursing Practice states that, “The psychiatric-mental health nurse provides, structures, and maintains a therapeutic environment in collaboration with the client and other health care clinicians.” II. Milieu, Defined A. Milieu therapy is defined as a scientific structuring of the environment to effect behavioral changes and to improve the psychological health and functioning of the individual. B. Within the therapeutic community setting, the client is expected to learn adaptive coping, interaction, and relationship skills that can be generalized to other aspects of his or her life. III. Current Status of the Therapeutic Community A. Milieu therapy came into its own during the time when hospital stays for psychiatric clients were extended. B. The current focus of care is on short stays and is often more biologically based. C. Strategies of milieu therapy have been modified to conform to the shortterm approach to care or to outpatient treatment programs. D. Some programs (e.g., those for children and adolescents, clients with substance addictions, and geriatric clients) have successfully adapted the concepts of milieu treatment to their specialty needs. IV. Basic Assumptions A. The health in each individual is to be realized and encouraged to grow. B. Every interaction is an opportunity for therapeutic intervention. C. The client owns his or her own environment. D. Each client owns his or her own behavior. E. Peer pressure is a useful and powerful tool. F. Inappropriate behaviors are dealt with as they occur. G. Restrictions and punishment are to be avoided. IV. Conditions that Promote a Therapeutic Community A. Basic physiological needs are fulfilled. B. The physical facilities are conducive to achievement of the goals of therapy. C. A democratic form of self-government exists. D. Responsibilities are assigned according to client capabilities. E. A structured program of social and work-related activities is scheduled as part of the treatment program. F. Community and family are included in the program of therapy in an effort to facilitate discharge from treatment. V. The Program of a Therapeutic Community A. The program is directed by an interdisciplinary team. B. A treatment plan is formulated by the team. C. Members of all participating disciplines sign the treatment plan and meet regularly to update the plan as needed. D. Disciplines may include psychiatry, psychology, nursing, social work, occupational therapy, recreational therapy, art therapy, music therapy, dietetics, and chaplain’s service. VI. Role of the Nurse A. Through use of the nursing process, nurses manage the therapeutic environment on a 24-hour basis. B. Nurses have the responsibility for ensuring that clients’ physiological and psychological needs are met. C. Nurses also are responsible for: 1. Medication administration 2. Development of a one-to-one relationship 3. Setting limits on unacceptable behavior 4. Client education