Krug l.m.-et-al.-2010-cancer-immunology-immunotherapy
DP KUL Poster final
1. B C
A
INTRODUCTION
• Neuroblastoma (NB) is a paediatric tumour of the sympathetic nervous system.
• It accounts for 15% of all deaths in childhood deaths due to cancer.
• About 50% of NB patients belong to the high-risk group, which have an overall
survival rate of <40%. Therefore novel therapeutic treatments are needed for
this large proportion of NB patients. Chk1 (check point kinase 1) is a protein
involved in the DNA damage response and plays a key role in activating cell
cycle checkpoints. Because it is over-expressed in several adult-type cancers,
anti-Chk1 compounds are in various phases of trials in adults with cancer.
• High Chk1 mRNA expression is reported in NBs1 However the level of Chk1
protein has not been studied at a tissue level.
CONCLUSIONS
• Increased expression of Chk1 protein correlated with key adverse clinical,
pathological and biological factors in NB samples.
• Higher expression in the high-risk group supports the use of anti-Chk1
agents in this group of patients with neuroblastoma.
AIM
To investigate Chk1 protein levels by immunohistochemistry in NB samples and
to assess the relationship between Chk1 levels and adverse prognostic factors.
METHODOLOGY
35 NB samples were stained with an anti-Chk1 antibody and stained sections
were digitized using Aperio ScanScope CS2 (Aperio Technologies, Inc., Vista,
CA, USA).
The proportion of NB cells expressing Chk1 protein (Figure 1a) was quantified
using Definiens Tissue Studio 4.0 in each sample (Figures 1b-1c).
REFERENCES:
1. Cole KA et al (2011) RNAi screen of the protein kinome identifies checkpoint kinase 1 (CHK1) as a therapeutic target in neuroblastoma. Proc Natl Acad Sci U S A 108:3336-3341
Contact: pajvd@bris.ac.uk
High Chk1 protein levels correlate with adverse prognostic factors in neuroblastoma
Hannah Turner 1,2, Emile Sowa-Avugrah 1, Urmila Uparkar 1,3, Pramila Ramani1,2
1Department of Histopathology, University Hospitals Bristol NHS Foundation Trust, Bristol Royal Infirmary, Bristol BS2 8HW, UK;
2 School of Cellular and Molecular Medicine, University of Bristol, School of Medical Sciences, University Walk, Bristol BS8 1TD, UK;
3 Department of Medical Oncology, Gujarat Cancer Research Institute, Asarwa, Ahmedabad, India 3800016.
Figure 1d: Screenshot showing selection of
cells expressing Chk1
Blue nuclei are negative for Chk1 whereas the
yellow nuclei represent brown nuclei in Figure 1c
that are stained by the anti-Chk1 antibody and
scored positive for Chk1 expression.
•Tissue sample with six regions of interest.•Tissue sample with six regions of interest.•Tissue sample with six regions of interest.
Figure 1b: Manual region
of interest (ROI) selection
Each ROI is represented by
a different colour. Tissue
sample with six ROIs.
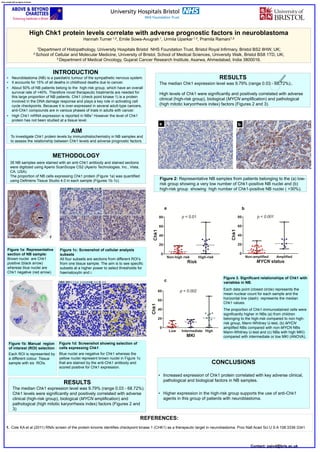
Figure 3. Significant relationships of Chk1 with
variables in NB.
Each data point (closed circle) represents the
mean nuclear count for each sample and the
horizontal line (dash) represents the median
Chk1 values.
The proportion of Chk1-immunostained cells were
significantly higher in NBs (a) from children
belonging to the high-risk compared to non high-
risk group, Mann-Whitney U-test, (b) MYCN
amplified NBs compared with non-MYCN NBs
Mann-Whitney U-test and (c) NBs with high MKI)
compared with intermediate or low MKI (ANOVA),
Figure 1c: Screenshot of cellular analysis
subsets
All four subsets are sections from different ROI’s
from one tissue sample. The aim is to see specific
subsets at a higher power to select thresholds for
haematoxylin and i.
Figure 1a: Representative
section of NB sample:
Brown nuclei are Chk1
positive (black arrow)
whereas blue nuclei are
Chk1 negative (red arrow).
RESULTS
The median Chk1 expression level was 9.79% (range 0.03 - 68.72%).
Chk1 levels were significantly and positively correlated with adverse
clinical (high-risk group), biological (MYCN amplification) and
pathological (high mitotic karyorrhexis index) factors (Figures 2 and
3)
RESULTS
The median Chk1 expression level was 9.79% (range 0.03 - 68.72%);.
High levels of Chk1 were significantly and positively correlated with adverse
clinical (high-risk group), biological (MYCN amplification) and pathological
(high mitotic karyorrhexis index) factors (Figures 2 and 3).
ba
Figure 2: Representative NB samples from patients belonging to the (a) low-
risk group showing a very low number of Chk1-positive NB nuclei and (b)
high-risk group showing high number of Chk1-positive NB nuclei ( >30%).
c
ba