Anamnese (englisch) Krankengeschichte
•
1 like•733 views

Krankengeschichte Patientinnen Frauenarztpraxis

Recommended
More Related Content
Similar to Anamnese (englisch) Krankengeschichte
Similar to Anamnese (englisch) Krankengeschichte (20)
More from Frauenarztpraxis Berlin-Mitte
More from Frauenarztpraxis Berlin-Mitte (8)
Recently uploaded
Recently uploaded (20)
Anamnese (englisch) Krankengeschichte
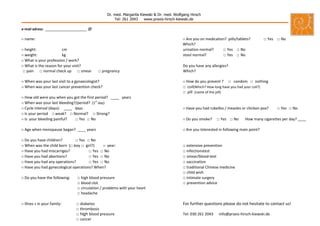
- 1. ++ Dr. med. Margarita Kiewski & Dr. med. Wolfgang Hirsch Tel: 261 2043 www.praxis-hirsch-kiewski.de e-mail adress: ____________________ @ o name: o Are you on medication? pills/tablets? □ Yes □ No Which? o height: cm urination normal? □ Yes □ No o weight: kg stool normal? □ Yes □ No o What is your profession / work? o What is the reason for your visit? Do you have any allergies? □ pain □ normal check up □ smear □ pregnancy Which? o When was your last visit to a gynaecologist? o How do you prevent ? □ condom □ nothing o When was your last cancer prevention check? □ coil(Which? How long have you had your coil?) □ pill (name of the pill) o How old were you when you got the first period? ____ years o When was your last bleeding?/period? (1st day) o Cycle interval (days): ____ days o Have you had rubellos / measles or chicken pox? □ Yes □ No o Is your period □ weak? □ Normal? □ Strong? o Is your bleeding painful? □ Yes □ No o Do you smoke? □ Yes □ No How many cigarettes per day? ____ o Age when menopause began? ____ years o Are you interested in following main point? o Do you have children? □ Yes □ No o When was the child born (□ boy □ girl?) o year: □ extensive prevention o Have you had miscarriges? □ Yes □ No □ infectionstest o Have you had abortions? □ Yes □ No □ smear/blood-test o Have you had any operations? □ Yes □ No □ vaccination o Have you had gynecological operations? When? □ traditional Chinese medicine □ child wish o Do you have the following: □ high blood pressure □ intimate surgery □ blood clot □ prevention advice □ circulation / problems with your heart □ headache o Illnes s in your family: □ diabetes For further questions please do not hesitate to contact us! □ thrombosis □ high blood pressure Tel: 030 261 2043 info@praxis-hirsch-kiewski.de □ cancer