Recommended

Recommended
More Related Content
Viewers also liked
Similar to Roth_San Antonio Breast Cancer Symposium 2010-Risk-Benefit Framework to Evaluate Gene-Expression Profiling in Early-Stage Breast Cancer: A Decision Model Developed in Collaboration with Stakeholders
Similar to Roth_San Antonio Breast Cancer Symposium 2010-Risk-Benefit Framework to Evaluate Gene-Expression Profiling in Early-Stage Breast Cancer: A Decision Model Developed in Collaboration with Stakeholders (20)
Roth_San Antonio Breast Cancer Symposium 2010-Risk-Benefit Framework to Evaluate Gene-Expression Profiling in Early-Stage Breast Cancer: A Decision Model Developed in Collaboration with Stakeholders
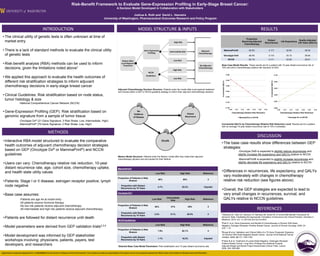
- 1. Risk-Benefit Framework to Evaluate Gene-Expression Profiling in Early-Stage Breast Cancer: A Decision Model Developed in Collaboration with Stakeholders Joshua A. Roth and David L. Veenstra University of Washington, Pharmaceutical Outcomes Research and Policy Program INTRODUCTION MODEL STRUCTURE & INPUTS RESULTS • The clinical utility of genetic tests is often unknown at time of Proportion market entry Receiving Adjuvant Distant Recurrences Life Expectancy Quality-Adjusted Life Years (QALYs) Chemotherapy • There is a lack of standard methods to evaluate the clinical utility MammaPrint® 50.0% 0.117 32.93 29.34 of genetic tests Oncotype Dx® 46.0% 0.110 33.10 29.50 NCCN 92.1% 0.111 33.09 29.41 • Risk-benefit analysis (RBA) methods can be used to inform Base Case Model Results: These results are for a patient with 10-year distant recurrence risk of decisions, given the limitations noted above1 15% and with a chemotherapy relative risk reduction of 25%. 0.080 0.100 • We applied this approach to evaluate the health outcomes of different risk stratification strategies to inform adjuvant 0.040 Incremental QALYs Incremental QALYs 0.096 chemotherapy decisions in early-stage breast cancer 0.000 0.092 Adjuvant Chemotherapy Decision Structure: Patients enter the model after local-regional treatment -0.040 and choose either a GEP or NCCN guideline strategy to inform their adjuvant chemotherapy decision. • Clinical Guidelines: Risk stratification based on node status, -0.080 0.088 tumor histology & size 0.084 -0.120 -National Comprehensive Cancer Network (NCCN) -0.160 0.080 0.05 0.10 0.15 0.20 0.25 0.30 0.35 0.05 0.10 0.15 0.20 0.25 0.30 0.35 • Gene-Expression Profiling (GEP): Risk stratification based on Chemotherapy Relative Risk Reduction Chemotherapy Relative Risk Reduction genomic signature from a sample of tumor tissue MammaPrint vs NCCN Oncotype Dx vs NCCN -Oncotype Dx® (21-Gene Signature; 3 Risk Strata: Low, Intermediate, High) -MammaPrint® (70-Gene Signature; 2 Risk Strata: Low, High) Incremental QALYs by Chemotherapy Relative Risk Reduction Level: Results are for a patient with an average 10-year distant recurrence rate of 15% if untreated. METHODS DISCUSSION • Interactive RBA model structured to evaluate the comparative • The base case results show differences between GEP health outcomes of adjuvant chemotherapy decision strategies strategies: based on GEP (Oncotype Dx® or MammaPrint®) and NCCN -Oncotype Dx® is expected to slightly reduce recurrences and guidelines slightly increase life expectancy and QALYs relative to NCCN Markov Model Structure: Patients enter the Markov model after they make their adjuvant chemotherapy decision and are tracked for their lifetime. -MammaPrint® is expected to slightly increase recurrences and • Users can vary: Chemotherapy relative risk reduction, 10-year slightly decrease life expectancy and QALYs relative to NCCN distant recurrence rate, age, cohort size, chemotherapy uptake, MammaPrint® and health state utility values • Differences in recurrences, life expectancy, and QALYs Low Risk High Risk Reference vary moderately with changes in chemotherapy Proportion of Patients in Risk • Patients: Stage I or II disease, estrogen receptor positive, lymph Stratum 50% 50% 3 relative risk reduction (see figures above) node negative Proportion with Distant 4.7% 25.3% Imputed Recurrence by 10 Years • Overall, the GEP strategies are expected to lead to • Base case assumes: Oncotype Dx® very small changes in recurrences, survival, and -Patients are age 44 at model entry Low Risk Intermediate Risk High Risk Reference QALYs relative to NCCN guidelines -All patients receive hormone therapy -No low risk patients receive adjuvant chemotherapy Proportion of Patients in Risk REFERENCES 54% 21% 25% 2 Stratum -All intermediate and high risk patients receive adjuvant chemotherapy Proportion with Distant 3.2% 9.1% 39.5% 2 1Veenstra DL, Roth JA, Garrison LP, Ramsey SD, Burke W. A Formal Risk-Benefit Framework for Recurrence by 10 Years • Patients are followed for distant recurrence until death Genomic Tests: Facilitating the Appropriate Translation of Genomics Into Clinical Practice. Genetics in Medicine. 2010; DOI: 10.1097/GIM.0b013e3181eff533. NCCN Guidelines 2Paik S. et al. Gene Expression and Benefit of Chemotherapy in Women With Node- Low Risk High Risk Reference • Model parameters were derived from GEP validation trials2,3,4 Negative, Estrogen Receptor–Positive Breast Cancer. Journal of Clinical Oncology. 2006; 24 (23): 1-12. Proportion of Patients in Risk 7.9% 92.1% 4 Stratum 3Buyse M et al. Validation and Clinical Utility of a 70-Gene Prognostic Signature • Model development was informed by GEP stakeholder Proportion with Distant for Women With Node-Negative Breast Cancer. Journal of the National Cancer Institute. 2006; 98(17): 1183-1192. 1.1% 16.2% Imputed workshops involving: physicians, patients, payers, test Recurrence by 10 Years 4Fisher B et al. Treatment of Lymph-Node-Negative, Oestrogen-Receptor- developers, and researchers Selected Base Case Model Parameters: Risk stratification and 10-year distant recurrence rate Positive Breast Cancer: Long-Term Findings from National Surgical Adjuvant Breast and Bowel Project Randomised Clinical Trials. Lancet. 2004; 364: 858-868. Supported by Cooperative Agreement No. 1U18GD000005 from the Centers for Disease Control and Prevention. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention.