GONIOMETRY GUIDE FOR RANGE OF MOTION MEASUREMENT
•Download as DOC, PDF•
4 likes•1,888 views


Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (13)
Similar to GONIOMETRY GUIDE FOR RANGE OF MOTION MEASUREMENT
Similar to GONIOMETRY GUIDE FOR RANGE OF MOTION MEASUREMENT (20)
Recently uploaded
Recently uploaded (20)
GONIOMETRY GUIDE FOR RANGE OF MOTION MEASUREMENT
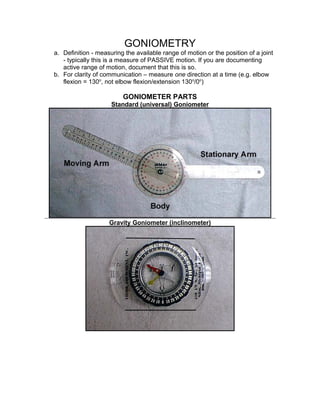
- 1. GONIOMETRY a. Definition - measuring the available range of motion or the position of a joint - typically this is a measure of PASSIVE motion. If you are documenting active range of motion, document that this is so. b. For clarity of communication – measure one direction at a time (e.g. elbow flexion = 130o , not elbow flexion/extension 130o /0o ) GONIOMETER PARTS Standard (universal) Goniometer Gravity Goniometer (inclinometer)
- 2. GONIOMETRY PROCEDURE a. Position joint in zero position and stabilize proximal joint component b. Move joint to end of range of motion (to assess quality of movement) c. Determine end-feel at point where measurement will be taken (at end of available range of motion) d. Identify and palpate bony landmarks e. Align goniometer with bony landmarks while holding joint at end of range f. Read the goniometer g. Record measurement (e.g. elbow flexion = 130o ) POSITIONING a. Start with joint at zero position - This is the reference point for the measurement. If zero position can't be achieved, this must be documented. b. permit complete range of motion 1) If you are assessing joint ROM, be sure that some other structure (eg. a tight muscle) doesn't interfere. 2) If you are assessing some other structure (eg. a tight muscle, pain limiting the motion) document exactly what is limiting the range of motion. (eg. hamstring tightness at 65o of hip flexion) STABILIZATION a. Poor stabilization is the most frequent cause of invlaid measurements. (eg. observe a "normal" ROM of elbow extension when movement of shoulder and arm masks a limitation - actually measuring shoulder and arm movement) Poor Stabilization for Elbow Extension
- 3. b. Usually stabilize proximal joint components c. Promote patient relaxation so voluntary muscle contraction doesn't interfere VALIDITY a. Validity is a measurement concept that asks whether a measurement system actually measures what it's supposed to (i.e., joint range of motion in the case of goniometry) b. Goniometric measurements can be invalid; usually because of poor stabilization. (See positioning and stabilization) RELIABILITY a. Reliability is a measurement concept that asks whether successive measurements are consistent, repeatable or reproducible. Upper extremity measurements are more reliable than lower extremity measurements. 1) Intratester reliability (same tester on different occasions)- measurement error should be less than 5 degrees 2) Intertester reliability (different testers) - measurement error probably greater than 5 degrees
- 4. b. To maximize reliability always use the same: 1) Goniometer 2) Positioning 3) Procedure 4) Examiner END FEEL a. The quality of resistance at end of range b. Each joint has a normal end feel at a normal point in the range of motion (ROM) c. Incorrect end feel, or correct end feel at incorrect ROM indicate pathology d. Terms: I suggest my terms for clarity of communication (to clearly identify the structure that the tester feels is limiting the ROM). Other authors use different terms - eg. hard, firm, soft, etc. I feel these "vague" terms lead to communication errors. Capsular - indicates that the joint capsule is limiting the ROM. Feels like stretching a leather belt. Example - knee extension. Ligamentous - indicates that ligament tightness is limiting the ROM. Feels like stretching a leather belt. Example - wrist radial deviation. Bony - indicates that bone touching bone is limiting the ROM. Feels like pushing two wooden surfaces together. Example - elbow extension.> Muscle Stretch - indicates that muscle tightness is limiting the ROM. Feels like stretching a bicycle tire innertube. Example - hip flexion while maintaining knee extension (straight leg raise) when hamstrings are tight. Soft Tissue Approximation - indicates that subcutaneous tissues (muscle bulk, fat) are pushing against each other and limiting the ROM. Feels like squeezing two balloons together. Example - calf pressing against thigh during knee flexion. Springy - indicates that a loose body is limiting the ROM. Feels "bouncy" like you are compressing a spring. Example - torn meniscal (knee) tissue limiting knee extension.
- 5. Empty - indicates that the examiner did not reach the end feel (usually the patient is not willing to allow motion to end of range because of anticipated pain). Feels like the joint has more range available, but the patient is purposefully preventing movement through the full ROM. Testing End Feel for Elbow Extension
- 6. EXTREMIDAD SUPERIOR SHOULDER FLEXION Test Position • Subject supine • Flatten lumbar spine (flex knees) • Shoulder no abduction, adduction or rotation • (Note: to measure gleno-humeral motion, stabilize scapula) Normal Range (For shoulder complex flexion) • 167o + or - 4.7o (American Academy of Orthopaedic Surgeons) • 150o (American Medical Association) • 166o (mean), 4.7o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – center of humeral head near acromion process • Stationary arm – parallel mid- axillary line • Moving arm – aligned with midline of humerus (lateral epicondyle) Normal End Feel • Muscle Stretch
- 7. EXTENSION DEL HOMBRO Test Position • Subject prone • Shoulder no abduction, adduction or rotation • (note: to measure gleno-humeral motion, stabilize scapula) Normal Range (for shoulder complex flexion) • 62o + or - 9.5o (American Academy of Orthopaedic Surgeons) • 50o (American Medical Association) • 62.3o (mean), 9.5o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – center of humeral head near acromion process • Stationary arm – parallel mid- axillary line • Moving arm – aligned with midline of humerus (lateral epicondyle) Normal End Feel • Capsular or ligamentous
- 8. ABDUCCION DEL HOMBRO Test Position • Subject supine • Shoulder 0o flexion and extension • Shoulder laterally (externally) rotated • Shoulder abducted • Stabilize thorax (note: to measure gleno-humeral motion, stabilize scapula) Normal Range (for shoulder complex abduction) • 184o + or - 7.0o (American Academy of Orthopaedic Surgeons) • 180o (American Medical Association) • 184o (mean), 7.0o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – center of humeral head near acromion process • Stationary arm – parallel to sternum • Moving arm – aligned with midline of humerus Normal End Feel • Muscle Stretch
- 9. ROTACION INTERNA DEL HOMBRO Test Position • Subject supine • Shoulder 90o abduction • Forearm neutral • Elbow flexed 90o • Stabilize arm Normal Range • 69o + or - 4.6o (American Academy of Orthopaedic Surgeons) • 90o (American Medical Association) • 68.8o (mean), 4.6o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – olecranon process of ulna • Stationary arm – aligned vertically • Moving arm – aligned with ulna (styloid process) Normal End Feel • Capsular
- 10. ROTACION EXTERNA DEL HOMBRO Test Position • Subject supine • Shoulder 90o abduction • Forearm neutral • Elbow flexed 90o • Stabilize arm Normal Range • 104o + or - 8.5o (American Academy of Orthopaedic Surgeons) • 90o (American Medical Association) • 103o (mean), 8.5o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – olecranon process of ulna • Stationary arm – aligned vertically • Moving arm – aligned with ulna Normal End Feel • Capsular
- 11. (styloid process) FLEXION DEL ANTEBRAZO Test Position • Subject supine • Shoulder neutral (arm at side) • Forearm supinated • Elbow flexed • Stabilize arm Normal Range • 141.0o + or - 4.9o (American Academy of Orthopaedic Surgeons) • 140.0o (American Medical Association) • 142.9o (mean), 5.6o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – lateral epicondyle of humerus • Stationary arm – aligned with humerus (center of acromion process) • Moving arm – aligned with radius (styloid process) Normal End Feel • Soft tissue approximation (capsular for thin subjects)
- 12. EXTENSION DEL CODO Test Position • Subject supine • Shoulder neutral (arm at side) • Forearm supinated • Elbow extended • Stabilize arm Normal Range • 0.3o + or - 2.0o (American Academy of Orthopaedic Surgeons) • 0.0o (American Medical Association) • 0.6o (mean), 3.1o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – lateral epicondyle of humerus • Stationary arm – aligned with humerus (center of acromion process) • Moving arm – aligned with radius Normal End Feel • Bone on bone
- 13. (styloid process) FOREARM SUPINATION Test Position • Subject sitting • Shoulder neutral (arm at side) • Elbow flexed to 90o • Stabilize arm • Supinate forearm Normal Range • 81o + or - 4.0o (American Academy of Orthopaedic Surgeons) • 80o (American Medical Association) • 82.1o (mean), 3.8o (standard
- 14. deviation), (Boone and Azen) Goniometer Alignment • Axis – medial to ulnar styloid • Stationary arm – parallel to humerus • Moving arm – aligned with ventral aspect of radius Normal End Feel • Capsular FOREARM PRONATION Test Position Normal Range
- 15. • Subject sitting • Shoulder neutral (arm at side) • Elbow flexed to 90o • Stabilize arm • Pronate forearm • 75o + or - 5.3o (American Academy of Orthopaedic Surgeons) • 80o (American Medical Association) • 75.8o (mean), 5.1o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – lateral to ulnar styloid • Stationary arm – parallel to humerus • Moving arm – aligned with dorsum of radius Normal End Feel • Capsular WRIST FLEXION Test Position • Subject seated • Forearm stabilized on table • Flex wrist (fingers relaxed) Normal Range • 75o + or - 6.6o (American Academy of Orthopaedic Surgeons) • 60o (American Medical Association)
- 16. • 76.4o (mean), 6.3o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – lateral wrist (triquetrum) • Stationary arm – aligned with ulna • Moving arm – aligned with fifth metacarpal Normal End Feel • Capsular WRIST EXTENSION Test Position • Subject seated • Forearm stabilized on table • Extend wrist (fingers relaxed) Normal Range • 74o + or - 6.6o (American Academy of Orthopaedic Surgeons) • 60o (American Medical Association) • 74.9o (mean), 6.4o (standard deviation), (Boone and Azen)
- 17. Goniometer Alignment • Axis – lateral wrist (triquetrum) • Stationary arm – aligned with ulna • Moving arm – aligned with fifth metacarpal Normal End Feel • Capsular WRIST RADIAL DEVIATION Test Position • Subject sitting with forearm resting on table • Stabilize forearm to prevent pronation or supination Normal Range • 21o + or - 4o (American Academy of Orthopaedic Surgeons) • 20o (American Medical Association) • 21.5o (mean), 4.0o (standard deviation), (Boon and Azen) Goniometer Alignment • Axis – capitate • Stationary arm – aligned with forearm (lateral epicondyle) • Moving arm – aligned with metacarpal of middle finger Normal End Feel • Ligamentous (ulnar collateral ligament)
- 18. WRIST ULNAR DEVIATION Test Position • Subject sitting with forearm resting on table • Stabilize forearm to prevent pronation or supination Normal Range • 35o + or - 3.8o (American Academy of Orthopaedic Surgeons) • 30o (American Medical Association) • 36.0o (mean), 3.8o (standard deviation), (Boon and Azen) Goniometer Alignment • Axis – capitate • Stationary arm – aligned with forearm (lateral epicondyle) • Moving arm – aligned with metacarpal of middle finger Normal End Feel • Ligamentous (radial collateral ligament) METACARPOPHALANGEAL JOINT FLEXION
- 19. Test Position • Subject sitting with forearm resting on table • Wrist and interphalangeal joints relaxed • Forearm neutral • Stabilize metacarpal to prevent motion Normal Range • 86o (index), 91o (long), 99o (ring), 105o (little) (American Academy of Orthopaedic Surgeons - active motion) • 90o (American Medical Association) Goniometer Alignment • dorsal metacarpophalangeal joint • Stationary arm – aligned with metacarpal • Moving arm – aligned with proximal phalange Normal End Feel • capsular
- 20. METACARPOPHALANGEAL JOINT EXTENSION Test Position • Subject sitting with forearm resting on table • Wrist and interphalangeal joints relaxed • Forearm neutral • Stabilize metacarpal to prevent motion Normal Range • 22o (index), 18o (long), 23o (ring), 19o (little) (American Academy of Orthopaedic Surgeons - active motion) • 20o (American Medical Association) Goniometer Alignment • dorsal metacarpophalangeal joint • Stationary arm – aligned with metacarpal • Moving arm – aligned with proximal phalange Normal End Feel • capsular
- 21. METACARPOPHALANGEAL JOINT ABDUCTION Test Position • Subject sitting with forearm resting on table • Wrist neutral • Forearm neutral • Stabilize metacarpal to prevent motion Normal Range • ??? Goniometer Alignment • dorsal metacarpophalangeal joint • Stationary arm – aligned with metacarpal • Moving arm – aligned with proximal phalange Normal End Feel • capsular
- 22. METACARPOPHALANGEAL JOINT ADDUCTION Test Position • Subject sitting with forearm resting on table • Wrist neutral • Forearm neutral • Stabilize metacarpal to prevent motion Normal Range • ??? Goniometer Alignment • dorsal metacarpophalangeal joint • Stationary arm – aligned with metacarpal • Moving arm – aligned with proximal phalange Normal End Feel • capsular
- 23. INTERPHALANGEAL JOINT FLEXION Note: This page demonstrates the technique for index proximal interphalangeal joint flexion. The technique for all other interphalangeal joints is similar. Simply align the goniometer over the proximal and distal joint partners (bones) for the joint you wish to measure. Test Position • Subject sitting with forearm resting on table • Wrist, metacarpal, and non-tested interphalangeal joints relaxed • Forearm neutral • Stabilize proximal bone to prevent motion Normal Range American Academy of Orthopaedic Surgeons • PIP fingers - 102o (index), 105o (long), 108o (ring), 106o (little) ( active motion) • DIP fingers - 72o (index), 71o (long), 63o (ring), 65o (little) ( active motion) • IP thumb - 73o American Medical Association • 100o (PIP fingers), 70o (DIP fingers), 80o (IP thumb) Normal End Feel
- 24. Goniometer Alignment • dorsal proximal interphalangeal joint • Stationary arm – aligned with proximal phalange • Moving arm – aligned with middle phalange Proximal Interphalangeal Finger Joints • bone on bone (if tissues overlying palmar aspect of bones is thin) • soft tissue approximation (if tissues overlying palmar aspect of bones is thick) Distal Interphalangeal Finger Joints and Thumb Interphalangeal Joint • capsular THUMB CARPOMETACARPAL JOINT FLEXION
- 25. Test Position • Subject sitting with forearm supinated and resting on table • Wrist neutral • Stabilize carpals to prevent wrist motion Normal Range • ??? Goniometer Alignment Normal End Feel
- 26. • Axis – carpometacarpal joint • Stationary arm – aligned with radius • Moving arm – aligned with metacarpal of thumb • Capsular THUMB CARPOMETACARPAL JOINT EXTENSION Test Position • Subject sitting with forearm supinated and resting on table • Wrist neutral • Stabilize carpals to prevent wrist motion Normal Range • ??? Goniometer Alignment • Axis – carpometacarpal joint • Stationary arm – aligned with Normal End Feel • Capsular
- 27. radius • Moving arm – aligned with metacarpal of thumb THUMB CARPOMETACARPAL JOINT ABDUCTION Test Position • Subject sitting with forearm resting on table • Wrist neutral • Forearm neutral • Stabilize carpals to prevent wrist motion Normal Range • 70o (American Academy of Orthopaedic Surgeons) Goniometer Alignment • Axis – radial styloid • Stationary arm – aligned with metacarpal of index finger • Moving arm – aligned with metacarpal of thumb Normal End Feel • Muscle stretch (adductor pollicus, skin, fascia)
- 28. THUMB CARPOMETACARPAL JOINT ADDUCTION Note: Thumb adduction is the return to neutral from thumb abduction. Thumb adduction is rarely measured, probably because it is rarely limited. Test Position • Subject sitting with forearm resting on table • Wrist neutral • Forearm neutral • Stabilize carpals to prevent wrist motion Normal Range • 0o ??? Goniometer Alignment • Axis – radial styloid • Stationary arm – aligned with metacarpal of index finger • Moving arm – aligned with metacarpal of thumb Normal End Feel • Soft tissue approximation THUMB CARPOMETACARPAL JOINT OPPOSITION
- 29. Note: Opposition of the thumb causes the pad of the thumb to face (oppose) the pads of the fingers. Opposition cannot be measured with a goniometer. The American Academy of Orthopaedic Surgeons suggests that opposition range is normal when the tip of the thumb can touch the base of the fifth finger. When range is not adequate, a ruler can be used to measure the distance between the tip of the thumb and the base of the fifth finger. Test Position • Subject sitting with forearm supinated and resting on table • Wrist neutral • Stabilize fifth metacarpal Normal Range • Able to touch tip of thumb to base of fifth finger (American Academy of Orthopaedic Surgeons) Goniometer Alignment • Goniometer cannot be used • Use a ruler to measure distance between tip of thumb and base of fifth finger Normal End Feel • Capsular or soft tissue approximation
- 30. EXTREMIDAD INFERIOR HIP FLEXION Test Position • Subject supine • Allow knee to flex (to avoid limitation by tight hamstrings) • Stabilize pelvis to prevent rotation • Flex hip Normal Range • 121.0o + or - 6.4o (American Academy of Orthopaedic Surgeons) • 100.0o (American Medical Association) • 122.3o (mean), 6.1o (standard deviation), (Boone and Azen)
- 31. Goniometer Alignment • Axis – greater trochanter • Stationary arm – aligned with midline of plevis • Moving arm – aligned with femur (lateral epicondyle) Normal End Feel • Capsular HIP EXTENSION Test Position • Subject prone • Stabilize pelvis to prevent rotation • Extend hip Normal Range • 12.0o + or - 5.4o (American Academy of Orthopaedic Surgeons) • 30.0o (American Medical Association) • 9.8o (mean), 6.8o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – greater trochanter Normal End Feel
- 32. • Stationary arm – aligned with midline of plevis • Moving arm – aligned with femur (lateral epicondyle) • Capsular or ligamentous HIP ABDUCTION Test Position • Subject supine • Stabilize pelvis to prevent pelvic list • Abduct hip Normal Range • 41.0o + or - 6.0o (American Academy of Orthopaedic Surgeons) • 40.0o (American Medical Association) • 45.9o (mean), 9.3o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – anterior superior iliac spine Normal End Feel
- 33. (ASIS) • Stationary arm – aligned with opposite ASIS • Moving arm – aligned with femur (center of patella) • Capsular or ligamentous HIP ADDUCTION Test Position • Subject supine • Stabilize pelvis to prevent pelvic list • Abduct opposite hip (to allow room for tested limb to adduct) • Adduct hip Normal Range • 27.0o + or - 3.6o (American Academy of Orthopaedic Surgeons) • 20.0o (American Medical Association) • 26.9o (mean), 4.1o (standard deviation), (Boone and Azen) Goniometer Alignment • Axis – anterior superior iliac spine Normal End Feel
- 34. (ASIS) • Stationary arm – aligned with opposite ASIS • Moving arm – aligned with femur (center of patella) • Capsular or ligamentous HIP MEDIAL (INTERNAL) ROTATION Test Position • Subject sitting on table • knee flexed • Stabilize distal thigh • medially (internally) rotate hip Normal Range • 44.0o + or - 4.3o (American Academy of Orthopaedic Surgeons) • 40.0o (American Medical Association) • 47.3o (mean), 6.0o (standard deviation), (Boone and Azen) Goniometer Alignment Normal End Feel
- 35. • Axis – center of patella • Stationary arm – aligned vertically • Moving arm – aligned with leg (crest of tibia) • Capsular HIP LATERAL (EXTERNAL) ROTATION Test Position • Subject sitting on table • knee flexed • Stabilize distal thigh • hip laterally (externally) rotated Normal Range • 44.0o + or - 4.8o (American Academy of Orthopaedic Surgeons) • 50.0o (American Medical Association) • 47.2o (mean), 6.3o (standard deviation), (Boone and Azen) Goniometer Alignment Normal End Feel
- 36. • Axis – center of patella • Stationary arm – aligned vertically • Moving arm – aligned with leg (crest of tibia) • Capsular KNEE FLEXION Knee flexion should be measured with the subject supine. This position allows assessment of the joint range of motion without interference from tightness in the rectus femoris muscle. If the examiner wishes to assess length of the rectus femoris, have the patient lie prone (see 2nd illustration). Test Position • Subject supine • Allow hip to flex • Flex knee Normal Range • 141o + or - 5.3o (American Academy of Orthopaedic Surgeons) • 150o (American Medical Association) • 142.5o (mean), 5.4o , (standard deviation) (Boone and Azen) Goniometer Alignment Normal End Feel
- 37. • Axis – lateral epicondyle of femur • Stationary arm – aligned with greater trochanter • Moving arm – aligned with lateral malleolus • Soft tissue approximation Supine Position (Rectus Femoris Limiting) KNEE EXTENSION
- 38. Test Position • Subject prone • Stabilize femur • Extend Knee Normal Range • minus 2.0o + or - 3.0o (American Academy of Orthopaedic Surgeons) Goniometer Alignment • Axis – lateral epicondyle of femur • Stationary arm – aligned with greater trochanter • Moving arm – aligned with lateral malleolus Normal End Feel • Capsular ANKLE DORSIFLEXION
- 39. Pronation of the sub-talar joint can compensate for a loss of ankle joint dorsiflexion range of motion. To avoid measurement error (by accidentally including sub-talar pronation), the sub-talar joint must be stabilized in its neutral position. To assess the range of JOINT motion, flex the knee (first illustration). To assess tightness of the gastrocnemius muscle, extend the knee (second illustration). Test Position • Subject prone • Flex knee • Stabilize sub-talar in neutral • Dorsiflex ankle by pushing through 5th metatarsal head Normal Range • 13o + or - 4.4o (American Academy of Orthopaedic Surgeons) • 20o (American Medical Association) • 12.6o (mean), 4.4o , (standard deviation) (Boone and Azen) Goniometer Alignment • Axis – lateral malleolus Normal End Feel • Capsular
- 40. • Stationary arm – aligned with fibular head • Moving arm – aligned with fifth metatarsal Assessing Gastrocnemius Tightness (muscle stretch end-feel) ANKLE PLANTARFLEXION
- 41. Test Position • Subject supine • Extend knee • Stabilize leg • Plantarflex ankle Normal Range • 56o + or - 6.1o (American Academy of Orthopaedic Surgeons) • 40o (American Medical Association) • 56.2o (mean), 6.1o , (standard deviation) (Boone and Azen) Goniometer Alignment • Axis – lateral malleolus • Stationary arm – aligned with fibular head • Moving arm – aligned with fifth metatarsal Normal End Feel • Capsular CALCANEAL INVERSION
- 42. Test Position • Subject prone • Stabilize tibia in sagittal plane (rotate hip or pelvis to align tibia) • Invert calcaneus Normal Range • 2/3 of total range from extreme of inversion to extreme of eversion should be inversion. About 20o inversion (and 10o eversion) on average (Seibel MO: Foot Function: A Programmed Text,p. 72, Baltimore, Williams & Wilkins, 1988) • 37.0o + or - 4.5o (American Academy of Orthopaedic Surgeons) Goniometer Alignment • Axis – automatically positioned by Normal End Feel
- 43. alignment of goniometer arms • Stationary arm – aligned with midline of leg • Moving arm – aligned with midline of calcaneus • Capsular CALCANEAL EVERSION Test Position • Subject prone • Stabilize tibia in sagittal plane (rotate hip or pelvis to align tibia) • Evert calcaneus Normal Range • 1/3 of total range from extreme of inversion to extreme of eversion should be eversion. About 10o eversion (and 20o inversion) on average (Seibel MO: Foot Function: A Programmed Text,p. 72, Baltimore, Williams & Wilkins, 1988)
- 44. • 21.0o + or - 5.0o (American Academy of Orthopaedic Surgeons) Goniometer Alignment • Axis – automatically positioned by alignment of goniometer arms • Stationary arm – aligned with midline of leg • Moving arm – aligned with midline of calcaneus Normal End Feel • Capsular MIDTARSAL INVERSION Test Position • Subject supine • Stabilize calcaneus and talus • Invert forefoot Normal Range • ??? Goniometer Alignment Normal End Feel
- 45. • Axis – automatically positioned by alignment of goniometer arms • Stationary arm – aligned with midline of leg • Moving arm – aligned with plantar aspect of metatarsal heads • Capsular MIDTARSAL EVERSION Test Position • Subject supine • Stabilize calcaneus and talus • Evert forefoot Normal Range • ??? Goniometer Alignment • Axis – automatically positioned by alignment of goniometer arms • Stationary arm – aligned with midline of leg • Moving arm – aligned with plantar Normal End Feel • Capsular
- 46. aspect of metatarsal heads METATARSOPHALANGEAL JOINT DORSIFLEXION (Extension) Range of first metatarsophalangeal (MTP) joint dorsiflexion is functionally important for gait. The available range of 1st MTP joint dorsiflexion depends on the position of the 1st ray. A plantarflexed 1st ray allows greater range of 1st MTP dorsiflexion. I recommend stabilizing the 1st ray in plantarflexion to measure maximum range of 1st MTP dorsiflexion. The first photo demonstrates a good method for measuring 1st or 5th MTP joint dorsiflexion by placing the goniometer alongside the bones. This technique cannot be used for the 2nd, 3rd, or 4th MTP joints. The second photo shows a technique for measuring these joints. Test Position • Subject supine • Stabilize 1st metatarsal in plantarflexion • Dorsiflex MTP Normal Range • 1st - 65o to 75o (slightly less at lesser MTPs) is the minimum required for normal gait (Root, Orien, Weed. Normal and Abnormal Function of the Foot, pp. 60-61, Clinical Biomechanics Corp., Los Angeles, 1977.) • 1st - 50o , 2nd - 40o , 3rd - 30o , 4th - 20o , 5th - 10o (American Medical Association)
- 47. Goniometer Alignment • Axis – medial to center of metararsal head • Stationary arm – aligned metatarsal • Moving arm – aligned with proximal phalange Normal End Feel • Capsular Assessing MTP Dorsiflexion by Placing Goniometer on Dorsum of Bones (requires modified goniometer) METATARSOPHALANGEAL JOINT PLANTARFLEXION (Flexion)
- 48. The first photo demonstrates a good method for measuring 1st or 5th MTP joint plantarflexion by placing the goniometer alongside the bones. This technique cannot be used for the 2nd, 3rd, or 4th MTP joints. The second photo shows a technique for measuring these joints. Test Position • Subject supine • Stabilize 1st metatarsal • Plantarflex MTP Normal Range • 1st - 30o , 2nd - 30o , 3rd - 20o , 4th - 10o , 5th - 10o (American Medical Association) Goniometer Alignment • Axis – medial to center of metararsal head • Stationary arm – aligned metatarsal • Moving arm – aligned with proximal phalange Normal End Feel • Capsular Assessing MTP Plantarflexion by Placing Goniometer on Dorsum of Bones (requires modified goniometer)
- 50. Test Position • Foot flat on table • Stabilize metatarsal • Abduct MTP Normal Range • ??? Goniometer Alignment • Axis – dorsum of center of metararsal head • Stationary arm – aligned with metatarsal • Moving arm – aligned with proximal phalange Normal End Feel • Capsular METATARSOPHALANGEAL JOINT ADDUCTION
- 51. Test Position • Foot flat on table • Stabilize metatarsal • Adduct MTP Normal Range • ??? Goniometer Alignment • Axis – dorsum of center of metararsal head • Stationary arm – aligned with metatarsal • Moving arm – aligned with proximal phalange Normal End Feel • Capsular COLUMNA VERTEBRAL
- 52. CERVICAL SPINE FORWARD BENDING (flexion) Test Position • Subject sitting with lumbar and thoracic spines supported • Stabilize lumbar and thoracic spines • Flex cervical spine Normal Range • 75.5o + or - 8.5o (20 - 29 yrs.), 70.5o + or - 17.5o (30 - 49 yrs.), 64.5o + or - 7o (>50 yrs.) (American Academy of Orthopaedic Surgeons) • 60o (American Medical Association) Goniometer Alignment • Axis – external auditory meatus • Stationary arm – vertical • Moving arm – aligned with nostrils Normal End Feel • Capsular or ligamentous CERVICAL SPINE BACKWARD BENDING (extension)
- 53. NOTE: The position of the mouth influences the available range of cervical backward bending. With the mouth closed, thghtness of the infrahyoid and suprahyoid muscles can limit range of cervical backward bending. If you wish to assess the range of the cervical spine, the mouth should be relaxed and slightly open. Test Position • Subject sitting with lumbar and thoracic spines supported • Stabilize lumbar and thoracic spines • Mouth relaxed and slightly open • Extend cervical spine Normal Range • 75.5o + or - 8.5o (20 - 29 yrs.), 70.5o + or - 17.5o (30 - 49 yrs.), 64.5o + or - 7o (>50 yrs.) (American Academy of Orthopaedic Surgeons) • 75o (American Medical Association) Goniometer Alignment • Axis – external auditory meatus • Stationary arm – vertical • Moving arm – aligned with nostrils Normal End Feel • Bony or Capsular CERVICAL SPINE SIDEBENDING
- 54. Test Position • Subject sitting with lumbar and thoracic spines supported • Stabilize lumbar and thoracic spines • Sidebend cervical spine Normal Range (unilateral) • 50.5o + or - 5.5o (20 - 29 yrs.), 46.5o + or - 6.5o (30 - 49 yrs.), 40o + or - 8.5o (>50 yrs.) (American Academy of Orthopaedic Surgeons) • 45o (American Medical Association) Goniometer Alignment • Axis – spinous process of C7 • Stationary arm – spinous processes of thoracic spine • Moving arm – posterior midline of head at occipital protuberance Normal End Feel • Capsular or ligamentous
- 55. CERVICAL SPINE ROTATION Test Position • Subject sitting with lumbar and thoracic spines supported • Stabilize lumbar and thoracic spines • Rotate cervical spine Normal Range (unilateral) • 91.5o + or - 5.5o (20 - 29 yrs.), 81o + or - 6.5o (30 - 49 yrs.), 77.5o + or - 7.5o (>50 yrs.) (American Academy of Orthopaedic Surgeons) • 80o (American Medical Association) Goniometer Alignment • Axis – center of superior aspect of head • Stationary arm – aligned with acromion processes • Moving arm – aligned with tip of nose Normal End Feel • Capsular or ligamentous
- 56. THORACO-LUMBAR SPINE FORWARD BENDING (flexion) TEST DE SHOBER NOTE: There are several methods for measuring the range of motion of the lumbar and thoracic spines. Each method has its own advantages and disadvantages (no method is completely valid or reliable, and normal values are not well established for any method). The method illustrated here is a good compromise. Take a baseline measurement with the patient standing upright, then take a second measurement with the subject in the forward bending position. Note the difference.
- 57. Test Position • Subject standing • Flex thoracic and lumbar spines Normal Range • 10 cm (Norkin and White) Tape Measure Alignment • Spinous processes of C7 and S1 Normal End Feel • Capsular or ligamentous
- 58. THORACO-LUMBAR SPINE BACKWARD BENDING (extenion) NOTE: There are several methods for measuring the range of motion of the lumbar and thoracic spines. Each method has its own advantages and disadvantages (no method is completely valid or reliable, and normal values are not well established for any method). The method illustrated here is a good compromise. Take a baseline measurement with the patient standing upright, then take a second measurement with the subject in the backward bending position. Note the difference.
- 59. Test Position • Subject standing • Extend thoracic and lumbar spines Normal Range • ??? Tape Measure Alignment • Spinous processes of C7 and S1 Normal End Feel • Capsular or ligamentous (sometimes bony) THORACO-LUMBAR SPINE SIDEBENDING
- 60. NOTE: There are several methods for measuring the range of motion of the lumbar and thoracic spines. Each method has its own advantages and disadvantages (no method is completely valid or reliable, and normal values are not well established for any method). The method illustrated here is a good compromise. Test Position • Subject standing • Stabilize pelvis • Sidebend thoracic and lumbar spines Normal Range (unilateral) • RIGHT: o 20 - 29 yrs 37.6o + or - 5.8o o 30 - 39 yrs 35.3o + or - 6.5o o 40 - 49 yrs 27.1o + or - 6.5o o 50 - 59 yrs 25.3o + or - 6.2o o 60 - 69 yrs 20.2o + or - 4.8o o 70 - 79 yrs 18.0o + or - 4.7o o (Fitzgerald, Wynveen, Rheault et al) • LEFT: o 20 - 29 yrs 38.7o + or - 5.7o o 30 - 39 yrs 36.5o + or - 6.0o o 40 - 49 yrs 28.5o + or - 5.2o o 50 - 59 yrs 26.8o + or - 6.4o o 60 - 69 yrs 20.3o + or - 5.3o
- 61. o 70 - 79 yrs 18.9o + or - 6.0o o (Fitzgerald, Wynveen, Rheault et al) • 25o (American Medical Association) Goniometer Alignment • Axis - S1 spinous process • Stationary arm - vertical • Moving arm - C7 spinous process Normal End Feel • Capsular or ligamentous ROTACION DEL TRONCO NOTE: There are several methods for measuring the range of motion of the lumbar and thoracic spines. Each method has its own advantages and disadvantages (no method is completely valid or reliable, and normal values are not well established for any method). The method illustrated here is a good compromise. Test Position • Subject sitting • Stabilize pelvis • Do not allow sidebending, forward bending or backward bending Normal Range (unilateral) • 45o (American Medical Association)
- 62. • Rotate thoracic and lumbar spines Goniometer Alignment • Axis - center of superior aspect of head • Stationary arm - aligned with anterior superior iliac spines • Moving arm - aligned with acromion processes Normal End Feel • Capsular or ligamentous TEMPEROMANDIBULAR JOINT OPENING Ruler Method Alternate Method
- 63. Test Position • Subject sitting • Stabilize cervical spine • Open Mouth Normal Range • 35 to 50 mm (Magee) • two and 1/2 flexed PIPs (Friedman and Weisberg) Ruler Alignment • Use a ruler to measure the distance between the upper and lower incisors • Alternate method - have the subject flex the proximal interphalangeal joints (PIPs) of the fingers and assess how many PIPs can fit between the teeth Normal End Feel • Capsular or ligamentous
- 64. TEMPEROMANDIBULAR JOINT PROTRUSION Test Position • Subject sitting • Stabilize cervical spine • Protrude mandible forward Normal Range • 3 to 5 mm (Magee) Ruler Alignment • Use a ruler to measure the distance between the upper and lower incisors Normal End Feel • Capsular or ligamentous
- 65. TEMPEROMANDIBULAR JOINT LATERAL DEVIATION Test Position • Subject sitting • Stabilize cervical spine • Deviate mandible laterally Normal Range • 10 to 15mm (Magee) Ruler Alignment • 1 - Identify points on the upper and lower teeth that are aligned when the mouth is in resting position (upper and lower incisors in this illustration) • 2 - Deviate the mandible laterally and use a ruler to measure the distance between the two points (upper and lower incisors in this illustration) Normal End Feel • Capsular or ligamentous