
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Cannabis Poster
Similar to Cannabis Poster (20)
Recently uploaded
Recently uploaded (20)
Cannabis Poster
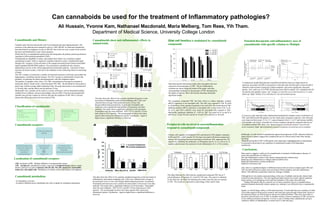
- 1. Ali Hussain, Yvonne Kam, Nathanael Macdonald, Maria Melberg, Tom Rees, Yih Tham. Department of Medical Science, University College London Can cannaboids be used for the treatment of Inflammatory pathologies? Data Showing the observations made when microglial cells were exposed to increasing doses of THC. The pro-inflammatory cytokines are shown along the bottom of the graph, with their corresponding %reduction in the presence of THC determined by the height of each bar. Bars with asterisks denoting statistically significant results. The exogenous compound THC has been shown to reduce inducible cytokine mRNA expression in rat microglial cells. The cells were exposed to THC (0.1mM to 10.0mM) for 24 hrs and then treated for 6 hrs with LPS. The results showed THC inhibited cytokine mRNA expression in microglial cells. Lower levels of IL-1a, IL-1b, IL-6, and TNF-a mRNAs were noted for microglial cells exposed to THC. Statistically significant inhibition ( P , 0.05) by THC was noted for IL-1a and IL-6 mRNAs at 1.0 and 10.0 μM, and for IL-1b and TNF-a mRNAs at 10.0 μM. Peripheral cells involved in neuroinflammation respond to cannabinoid compounds T-helper cells regulate cell mediated (Th1) and humoral (Th2) adaptive immunity. In MS and EAE, a shift towards Th1 has been associated with disease progression, whereas Th2 phentotype has been described as beneficial. THC suppresses the Th1 response by inhibiting the production of IFNgamma and IL-12, as well as IL-12 receptors and increases the expression of anti-inflammatory IL-4, a Th2 cytokine. Glial cell functi on is modulated by cannabinoid compounds This Data Illustrates the effect that the cannabinoid compound THC has on T cell proliferation, IFNgamma, IL-4 and Th1/Th2 ratio. The control is indicated by the white bar, the black bar indicating the results when the cells are exposed to THC. The results are expressed as a percentage of the control value. Cannabinoids and History Cannabis sativa has been historically used for recreational and rope-making purposes. The existence of the plant has been reported as early as 1500-1200 BC in China and cannabis has been described as an analgesic as early as 200 AD. Due to this for eons, in parts of the world it has been used medicinally to treat various diseases. Within the 60 or so cannabinoids produced by this hemp plant, the primary potent psychoactive ingredient is D9∆-tetrahydrocannabinol (THC). Cannabinoids are lipophillic in nature, and mediate their effects via a G-protein coupled cannabinoid receptor, which is negatively coupled to adenylyl cyclase. Cannabinoids signal through CB-1 receptors via the activation of the mitogen activated protien kinase/extracellular signal-regulated (MAPK/ERK) pathway. The psychoactive cannabinoids also increase dopaminergic activity in the ventral tegmental area-mesolimbic pathway. Activation of these neurones are known to play a vital role in the mediation of the reinforcing effects of most drugs of abuse. The CB-1 receptor is localised to a number of functional structures in the brain, particularly the hippocampus, cerebellum and the striatum. The CB-2 receptor is preferentially found in the periphery, in particular the spleen and haemopoietic cells (the lymphoid organs). The potency of cannabis varies, from 1-2% THC concentration in homegrown cannabis to chemically altered “skunk-weed”, which has about 50% THC. The threshold for intoxication is about 2mg, with the average spliff containing 25mg. The peak intoxication is not reached until 15-30 mins after, and the effects can last between 2-6 hrs. Medicinally wise, cannabis can be used for a variety of diseases, such as rheumatoid arthritis, irritable bowel syndrome, anorexia and multiple sclerosis (MS). It has been documented that cannabis may provide a means by which to alleviate the symptoms of MS. MS is a chronic disease that affects the central nervous system (CNS). Potential therapeutic anti-inflammatory uses of cannabinoids with specific relation to Multiple Messages from these studies A randomized, double-blind placebo-controlled trial failed to detect an improvement on spasticity associated with MS as measured by Ashworth scale, but did result in some benefit in subjective improvement of spasticity-related symptoms: pain (most significant), sleep and spasms. Also, orally use of Δ-9THC did decrease time walk by median 12%, compared with 4% for placebo and cannabis extract. Left: Changes in Ashworth scores from baseline to 13 weeks follow-up; Right: Median 10 m walk times by visit and treatment group A crossover study indicated orally administrated standardized cannabis extract (combination of THC and CBD) benefit MS patients over the whole study compared to placebo, with Ashworth score improved from mean 13.3 to 11.1; spasm frequency from 1.1 to 0.7 and increase mobility with tolerable side effects. Generally low toxicity symptoms are shown compared with the use of synthetic/isolated THC alone. Left: Spasm-frequency-protocol in patients received early active treatment; Right: Spasm-frequency-protocol in patients received late active treatment Data seems to suggest a viable use for cannabinoids in treatment of inflammatory diseases. It seems that cannabinoids are effective in: The anti-inflammatory actions in the murine carregeenan paw oedema assay Reducing joint inflammation in collagen induced arthritis mice. Reducing inflammatory cytokine production. Inhibition of Immune cells. Also, there is a significant degree or difference between the two known receptor types CB1 and CB2, the latter being the receptor most associated with the periphery and anti-inflammatory effects. This difference means that selectivity of drugs is feasible. Although the in vitro studies seem promising, in the case of multiple sclerosis the clinical trials seemed less than satisfactory. The only significant improvement was in pain. Muscle spasticity improvements were ambiguous at best and the limitations of the study incur difficulty. Finding MS patients that fit a specific set of criteria, and allow for use of cannabinoids as potential treatment drastically reduces sample size, making it very difficult to have a reproducible study. Finally, as with all drugs, safety is of the utmost priority. It seems that there are a number of viable CB receptor agonists being used in research, and some have gone through clinical trials. However the long term effects are still not known and are not without problems. There have been links to psychosis with the heavy use of THC in cannabis smokers, however analogues of THC are known to not exhibit psychoactive properties. It is now a case of whether these cannabinoids can have conclusive effects on inflammation, in which case it is still early days. Classification of canabinoids: Localization of cannabinoid receptors Cannabinoid receptors: This data shows the effect of two separate cannabinoid agonists on the movement of inflammatory and immune mediating cells. Cells were collected from a lavage of the peritoneal cavity of mice with thioglycollated induced peritonitis. In particular Neutrophils and monocytes were counted, the total number of leucocytes were then analysed. The results show a significant reduction in cell movement. Neutrophils show the most inhibition. WIN 55212-2 and HU-210 are both selective CB-2 agonists. The second graph set shows how these agonist effect monocytes chemotactic protein-1 production. Again in higher doses a significnnt inhibition is observed. This data shows the effect of two separate cannabinoid agonists on the movement of inflammatory and immune mediating cells. Cells were collected from a lavage of the peritoneal cavity of mice with thioglycollated induced peritonitis. In particular Neutrophils and monocytes were counted, the total number of leucocytes were then analysed. The results show a significant reduction in cell movement. Neutrophils show the most inhibition. WIN 55212-2 and HU-210 are both selective CB-2 agonists. The second graph set shows how these agonist effect monocytes chemotactic protein-1 production. Again in higher doses a significnnt inhibition is observed. ● Although, it is still unclear if cannabinoids oppose the progression of MS, subjective/objective improvement in spasms suggest that cannabinoids may be clinical useful when other therapy has failed. ● Significant benefit of THC in MS patient with central pain, highlighting that its amelioration is associated with protective up-regulation of cannabinoid receptor (CB2-dependent mechanism) Cannabinoids show anti-inflammatory effects in animal trials. CB1- localized to CNS Mediate inhibition of nerutransmitter release. CB2 - ‘peripheral’ cannabinoid receptor, expressed in lymphoid tissues (spleen, tonsils, thymus, pancreas etc) and on immune cells (B cells, NK cells, monocytes, neutrophils, leukocytes, microglial cells ) Modulation of cytokine release and immune cell migration. Cannabinoid metabolism : - by degradative enzymes - by passive diffusion across membranes into cells or uptake by membrane transporters Conclusions.