2. INTRODUCTION
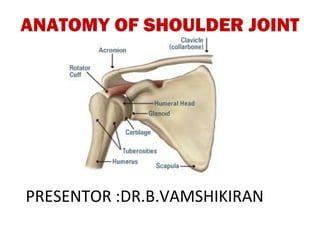
• Shoulder girdle is formed by scapula and clavicle
and humerus upper end.
• The only skeletal connection of upper limb to trunk
is clavicle[scapula is connected only through
muscular attachments].
• Shoulder area include-
-gleno humeral
-acromio clavicular
-scapulo thoracic
-sterno clavicular
3. • Surface anatomy land marks
• Joint structures.
• Ligaments and tendons.
• Relations ,muscles and nerves.
• Blood supply.
• Bursae around shoulder joint
• Range of movements.
• Applied anatomy.
4. SURFACE ANATOMY
• Anteriorly -Clavicle
-Tip of coracoid process of scapula
-Greater tubercle of humerus.
-Deltoid contour
-axilla and its folds
-medial epicondyle shows head of humerus direction
-lateral epicondyle show greater tuberosity direction
• Posteriorly –Scapula-acromian,crest of spine[T3]
medial and lateral borders,inferior angle
6. BONES
• Clavicle-Lateral end
• Scapula
• Upper end of humerus
• Superior shoulder
suspensory complex-it
is a group of bony and ligamentous attachments
includes coracoid,acromian,glenoid,distal
clavicle,coracoclavicular ligament[main bond
b/w scapula and clavicle].
• Superior strut by middle 1/3rd clavicle a
• Inferior strut by lateral scapular body and spine
7. OSSIFICATION CENTRES
• PROXIMAL HUMERUS-3 ossification centre.
• Humeral head-ossifies at 6mths
• Greater tuberosity-ossifies at 1 to 3yrs
• Lesser tuberosity-ossifies at 4 to 5yrs.
• Tuberosities coalesce at 6to 7yrs and
then fuses to humeral head 7 to13yrs.
• Physis close at 14-17yrs girls and 16-18yrs boys.
• Proximal physis is extra-articular except at medial
aspect
8. OSSIFICATION CENTRES
• CLAVICLE-It’s the 1st bone to ossify .
• It has no medullary cavity.
• It occurs by intramembranous ossification.
• Secondary ossification centres via endochondral.
• Medial epiphysis ossifies at 12-19yrs and fuses at 22
to 25yrs.
• Lateral epiphysis ossifies and fuses at 19yrs.
• It is most commonly #long bone in body.
10. OSSIFICATION CENTRES
• SCAPULA-body,spine,coracoid,acromian,glenoid
-Body and spine[posterior] ossify at birth
-Coracoid process[anterior]-atavastic epiphysis.
- centre at1yr,base at 10yrs,tip at variable
- all 3 fuse by 15-16yrs.
-Acromian[lateral projection]-fuses by 22yrs via
2- 5centres form at puberty
-Glenoid-upper1/4th ossify at 10yrs
-lower3/4th appear at puberty ,fuse by22
11. ACROMIOCLAVICULAR JOINT
• Its a plane synovial joint formed by articular facets
of lateral end of clavicle and medial acromial
margin
• Cavity of joint is subdivided ay ARTICULAR DISC
which may be perforated
• Blood supply-
suprascapular
thoracoacromial
[br. of axillary artery]
12. SHOULDER JOINT
• It’s multiaxial synovial ball and socket[dish]joint.
• In anatomical position -
-Glenoid articular surface has 7*posterior version
-Proximal end of humerus is 45*tilted upwards
vertical angle with long axis of humerus and 20*
RETROVERTED with reference to transverse distal
intercondylar line.
-Scapula is 30*anterior to body’s transverse plane
• The humeral retroversion is 27* right and 21*left
• Anatomical neck and surgical neck
13. • Glenoid cavity diameters-
-transversely-24+/-3mm
-superioinferiorly-35+/-4mm
-radius curvature 36+/-7mm
-articular surface is PEAR shaped due to anterior
incisura acetabuli and relatively small and flat.
-only 1/4th of humeral head is in contact with glenoid
cavity hence greater mobility is seen.
14. JOINT STABILITY
Passive mechanisms like Active mechanisms like
• Joint confirmity • Musculo-tendinious
• Vacum effect of rotator cuff[dynamic
limited joint volume stabiliser]
• glenoid labrum • Muscles attaching limb
[static stabiliser] to thorax like pectoralis
• joint capsule major
• Long head of BICEPS
• glenohumeral
and TRICEPS
ligaments
• coracoacromial
arch[osseo-
ligamentous arch]
• Scapular inclination
16. GLENOID LABRUM
• It’s a fibrocartilagenous rim attached to margin of
glenoid cavity and inc concavity by 50% and suface
area of humeral attachment by 75%.
• It further strengthens by long head of biceps origin
and sup glenohumeral ligament
• It is a STATIC stabiliser of joint and prevents
excessive rollback of humerus
17. JOINT CAPSULE
• It is lax and attaches along epiphyseal lines of
glenoid and humeral head and extends onto
surgical neck medially.
• Capsule is surrounded by synovial
membrane which prolongs along
tendon of biceps as tubular sheath
• Inf part weakest-resulting in dislocations
• APPLIED ANATOMY-OSTEOMYELITIS of humerus
upper end spreads directly to joint due to capsule
extension to medial side of neck
18. RELATIONS OF ARTICULAR CAPSULE
• MEDIALLY-beyond supraglenoid tubercle
andlabrum
• LATERALLY-attaches to anatomical neck of humerus
• INFERIORLY-attachment extends to surgical neck
• SUPERIORLY-deficient for biceps long head passage
• ANTERIORLY-reinforced by GLENOHUMERAL
LIGAMENTS[sup,middle,inf]
19. GLENOHUMERAL LIGAMENTS
• SUPERIOR-It is the most superior capsular
thickening from labrum anterior to long head of
biceps at level of coracoid base
• It passes under supraspinatus and inserts on
ANATOMICAL NECK medial to anterosuperior base
of lesser tuberosity.
20. • MIDDLE GLENOHUMERAL-most variable in size
• Arises just inferior to superior GHL and inserts along
middle area of ANATOMICAL NECK opposite to
lesser tuberosity
21. • INFERIOR GLENOHUMERAL-It’s the THICKEST part
• It is very broad arising from lower half of
labrum[anterior,inferior,posterior]
• Thick superior margin is called SUPERIOR BAND,
rest of it is called AXILLARY POUCH.
• Superior band and anterior pouch insert on
ANATOMICAL NECK while the posterior pouch on
SURGICAL NECK
22. APPLIED ASPECTS OF GLENOHUMERAL LIGAMENTS
• They restrain the selective arcs of abduction and
external rotation.
• In arm dependent position all are slack.
• The SUPERIOR GHL is primary resistrant to
inferior translation of adducted shoulder
• The MIDDLE GHL limits external rotation at 45*
of abduction
• The INFERIOR GHL limits external rotation at 45
to 90* of abduction[mainly superior band of it].
23. • CORACOHUMERAL LIGAMENT-arises from lateral
base of coracoid process and extends onto both
tuberosities.
• It forms roof of bicipital
tendon sheath and
strengtens capsule anteriorly
Importance-resists inferior and posterior translation.
• TRANSVERSE HUMERAL LIGAMENT-bridges upper
part of bicipital groove through which long head of
biceps passes down.
24. CORACOACROMIAL LIGAMENT
• It’s a trapezoidal ligament from base of acromian to
apophysis of coracoid
• It along with coracoid
and acromian forms
CORACOACROMIAL ARCH
which is a
SECONDARY SOCKET
to humerus head.
• It plays role in resisting upward displacement of
humerus
25. CORACOCLAVICULAR LIGAMENT
• Very strong ligament from outer and inferior
clavicular surface to coracoid base
• 2components-CONOID and TRAPEZOID
• IMP FUNCTION-It is prime suspensory ligament of
upper extremity that couples”glenohumeral
abduction and flexion”to”scapular rotation on
thorax”.
• Conoid portion is primary restraint to anterior and
superior rotation and anterior and superior
displacement of clavicle
• Trapezoid has relatively less role than conoid part
26. BURSAE RELATED TO SHOULDER JOINT
• SUBACROMIAL BURSA-protect suprspinatus
• SUBSCAPULARIS BURSA
• INFRASPINATUS BURSA
27. RELATIONS OF SHOULDER JOINT
• SUPERIORLY-
coracoacromial arch,
subacromial bursa,
supraspinatus,deltoid
• INFERIORLY-
long head of triceps
• ANTERIORLY-subscapularis,coracobrachialis
biceps short head,deltoid[ant fibres]
• POSTERIORLY-infraspinatus,teres minor,deltoid
• WITHIN JOINT-Long head of biceps
29. NERVE SUPPLY
• Axillary nerve-passes close to surgical neck of
humerus abt 5cm below acromian
• Musculocutaneous nerve
• Suprascapular nerve-Just passes over clavicle
30. PRINCIPAL MUSCLES AROUND SHOULDER
• Primary role -a.movements of arm
b.dynamic stabilisation of glenohumeral joint.
• There are 14 muscles which are divided into 4
functional groups.they are
1.Three heads DELTOID[anterior,middle,posterior]
2.Four rotator cuff muscles and BICEPS muscle
3.Two axiohumeral muscles[PECTORALIS MAJOR and
LATTISMUS DORSI] and TERES MAJOR.
4.Scapular muscle group –SERRATUS
ANTERIOR,TRAPEZIUS,RHOMBOID MAJOR and
MINOR and LEVATOR SCAPULAE
32. • SCAPULA POSTERIOR ANTERIOR
supraspinatus subscapularis
infraspinatus
Teres minor
33. MUSCLE ORIGIN INSERTION NERVE SUPPL ACTION
DELTOID-4septa origin Deltoid Axillary Acromial fibres-abductors
Ant border lat 1/3rd clavicle tuberosity on nerve[c5,6] From90*
Acromian lateral border humerus Anterior fibres-flexors and
Lower lip crest of spine of medial rotators
scapula Posterior fibres-extensors
and lateral rotators
SUPRASPINATUS-medial2/3 Greater Suprascapular Initiator of
Of supraspinatus fossa tubercle nerve[c5,6] abduction0*15*
upperimpresi steadies
humeralhead
INFRASPINATUS-medial2/3 Greater Suprascapular Lateral rotator of arm
of infraspinatus fossa tubercle nerve[c5,6]
TERES MINOR-Upper2/3 of Greater Axillary Lateral rotator of arm
dorsal surface of scapula tubercle nerve[c5,6]
SUBSCAPULARIS-medial 2/3 Lesser Upper ,lower Medial rotator and
of subscapular fossa tubercle subscapular N adductor of arm
BICEPS- Radial Musculocutan Strong supinator when
Short head-tip of coracoid tuberosity of eous forearm flexed
Long head-supraglenoid posteriorly nerve[c5,6] Flexor of elbow
Short head-arm flexor
Long head-prevents
upward displacement
34. MUSCLE ORIGIN INSERTION NERVE SUPPLY ACTION
PECTORALIS MAJOR Bilaminar tendon on Medial and Adduction and medial
Ant surface of clavicl lateral lip.two lamina lateral pectoral rotation of shoulder
Ant manubrium[ant are continous nerve Clavicular-arm flexor
lamina] Fibres from sternum Sternoclavicular part-
• Table of page 143 chaurasia
2nd-6th coastal cartilage and aponeurosis are extension of flexed
External oblique twisted and inserted arm against resistance
abdominus
aponeurosis[post lamin]
LATTISMUS DORSI- Winds round lower Thoracodorsal Adduction,extension,
Outer lip of iliac crest border of teres major nerve[c6,7,8] medial rotation of
post 1/3rd and forms posterior shoulder
Posterior layer of axillary fold Helps in voilent
lumbar fascia Tendon is twisted expiratory effort
T7-12 spinous process upside down insert Climbing muscle
Lower 4ribs into intertubercular Holds inferior angle of
Inf angle scapula sulcus of humerus scapula in place
TERES MAJOR- Medial lip of bicipital Lower Medial rotator and
Lower 1/3rd of dorsal groove subscapular adductor arm
surface of lateral and nerve[c5,6]
inferior angle scapula
37. MUSCLE ORIGIN INSERTION NERVE SUPPLY ACTION
SERRATUS ANTERIOR- Coastal surface of Nerve to serratus Pulls scapula forward
8digitations of upper scapula medial border anterior c5,6,7 around chest wall to
8ribs 1st digitation sup angle to protract limb
root of spine Inf fibres-pull it forward
Next two-medial border and rotate
Lower 5-inferior angle Steadies scapula
Forced inspiration
TRAPEZIUS- Upper fibres-posterior Spinal part of Upper fibres[+LS]-
Medial 1/3 of superior border of clavicle lat 1/3 accesory nerve- elevate scapula
nuchal line Middle fibres-medial motor Middle fibres[+R]-
External occipital margin acromian and C3,4-proprioceptive retract scapula
protuberance upper lip crest of spine Lower fibres[+SA]-
Ligamentum nuchae of scapula rotate scapula forwards
C7 spine ;arm abductio beyond
T1-12 spines 90*
Steadies scapula
RHOMBOIDES MINOR- Base of triangular area at Dorsal scapular Retraction of scapula
Ligamentum nuchae root of spine of scapul nerve[c5]
Spines c7-T1
RHOMBOIDES MAJOR Medial border of scapula Dorsal scapular Retraction of scapula
below of root of spine nerve[c5]
LEVATOR SCAPULA
38. MUSCLE ORIGIN INSERTION NERVE ACTION
LEVATOR SCAPULA- Superior angle and Branch of dorsal Elevation of scapula
Transverse process upper part of medial scapular nerve[c5] Steadies scapula
of c1,2 border of scapula during arm
Posterior tubercles movements
of transverse
process of c3,4
39. MOVEMENTS AROUND SHOULDER
• Shoulder movements occur by coordinated
motions of –
1. Clavicular and sternoclavicular
2. Acromioclavicular motion
3. Scapulothoracic motion
4. Glenohumeral motion
40. CLAVICULAR AND STERNOCLAVICULAR MOTION
• At sternoclavicular joint,clavicle rises slow and
steadiely 30* with 90* of arm elevation
• Clavicular protraction ,retraction also occurs
• the clavicle rotates 45* on its long axis during
elevation of arm to full overhaed position180*.
ACROMIOCLAVICULAR MOTION
• It provides only two small arcs of motion about
15* during first and last 40* of arm elevation.
• Clavicular rotation is essential for terminal arc
mobility of acromioclavicular joint
41. SCAPULOTHORACIC MOTION
• Its not a true joint but scapula glides freely on the
loose aereolar tissue between two surfaces
• Direction of movement described by acromian
motion and sternoclavicular joint integrity
• Rotation of scapula is facilitated by
sternoclavicular and acromioclavicular joints
42. SCAPULA MOVEMENTS
• Elevation - moving the superior border of the scapula and the
acromion in an upward direction.
• Depression - moving the superior border of the scapula and
the acromion in an downward direction.
• Upward Rotation - Moving the scapula so that the glenoid
cavity faces upward.
• Increases the ranges of motion during abduction and/or
flexion of the shoulder.
• Downward Rotation - moving the scapula so that the glenoid
cavity faces inferiorly.
• Increases range of motion during extension and / or
adduction of the shoulder.
• Protraction ( Abduction)- moving the scapula away from
midline
• Retraction (Adduction) - moving the scapula toward midline
43. SCAPULOTHORACIC MOTION
MOVEMENT MUSCLE
VERTICAL PLANE Upper fibres of trapezius Infero lateral compartment
ELEVATION Levator scapulae
DEPRESSION Lower fibres of serratus Infero lateral compartment
anterior and p.minor
HORIZONTAL PLANE Serratus anterior and Superomedial compart.
PROTRACTION-moving pectoralis minor Seen in pushing or
away from vertical spine punching actions
RETRACTION-moving Rhomboides and middle Superomedial
towards vertical spine trapezoid fibres compart.seen in squarring
of shoulders
FORWARD ROTATION- Trapezius upper fibres Inferolateral compartment
occurs in arm over head Serratus ant lower fibres
abduction
BACKWARD ROTATION Rhomboides and levator Inferolateral compartment
scapula
44. GLENOHUMERAL MOTION
• Arm elevation is classified by its plane of action
• Flexion ,extension in SAGITTAL PLANE
• Abduction adduction in CORONAL/FRONTAL PLANE
• Medial and lateral rotations with a midflexed elbow
• CIRCUMDUCTION-combination of different
movements by which arm moves in circle
45. MOVEMENTS OF THE GLENOHUMERAL JOINT
– Movements of the shoulder joint (glenohumeral
joint) usually involve moving the humerus on the
scapula.
– All movements are to be studied starting from the
ANATOMICAL POSITION
– Axis of motion
• Flexion - Extension
– Coronal axis through head of humerus
• Abduction /Adduction
– Sagittal axis through humeral head
• Rotation
– Longitudinal axis through shaft of humerus
48. • Flexion moving the humerus forward and upward in the sagittal plane.
• Extension - bringing the arm down to the side in the sagittal plane.
• Abduction - moving the arm in the coronal plane away from the midline
– Stage-initiate -supraspinatus
15*-90*- deltoid
90*-180* - deltoid with upward rotation of scapula
• Adduction - moving the arm in the coronal plane towards the midline.
• Inward Rotation - rotating the arm in a transverse plane so that the
anterior surface of the bone turns inward.
• Outward Rotation - rotating the arm in a transverse plane so that the
anterior surface of the bone turns outward.
49. PRINCIPLE MUSCLES ACTING ON SHOULDER
MOVEMENTS MAIN MUSCLE ACCESSORY MUSCLE
FLEXION PECTORALISMAJOR(clavicular part) Coracobrachialis
0-135* DELTOID ant fibres Biceps short head
EXTENSION DELTOID post fibres Teres major
45-60* LATISSMUS DORSI Triceps long head
P major[sternocoastal head]
ADDUCTION PECTORALIS MAJOR Teres major
LATISSMUS DORSI coracobrachialis
BICEPS long head
TRICEPS short head
ABDUCTION SUPRASPINATUS[0-15*]
DELTOID[15*-90*]
SERRATUS ANTERIOR[90*-180*]
TRAPEZOIDupper,lower fibres[90-
180]
MEDIAL ROTATION PECTORALIS MAJOR subscapularis
[INTERNAL] DELTOID ant fibres
90* LATISSMUS DORSI
TERES MAJOR
LATERAL ROTATION DELTOID posterior fibres
[EXTERNAL] INFRASPINATUS
50. • Scapulohumeral Rhythm-Coordinated
movements of the scapula and the humerus
increasing the range of motion at the
glenohumeral joint
– Most noticeable during complete flexion and
abduction of the shoulder
– 2 * of humeral abduction is associated with 1* of
scapula rotation
• Humerus and scapula move in 2:1 ratio during
abduction
• For every 15* of elevation 10* occur at shoulder
joint and 5* by scapular movements
51. • ABDUCTION-
• Humeral head permits only upto 90*
• By scapula rotaion making glenoid cavity facing
ouwards the abduction range increased to 180
• This is brought about
serratus anterior and
trapezius
52. REFERENCES
• Text book of upperlimb-chaurasia
• Operative orthopaedics-campbell
• Hand book of fractures-zuckerman
• Manual of clinical surgery-Das
![INTRODUCTION
• Shoulder girdle is formed by scapula and clavicle
and humerus upper end.
• The only skeletal connection of upper limb to trunk
is clavicle[scapula is connected only through
muscular attachments].
• Shoulder area include-
-gleno humeral
-acromio clavicular
-scapulo thoracic
-sterno clavicular](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)