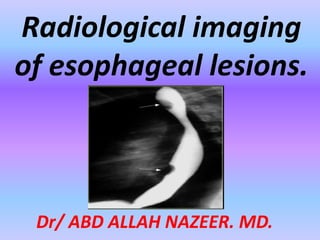
21. EPIPHRENIC DIVERTICULUM
•Arises in the distal
of the esophagus,
just above diaphragm
•Pulsion diverticulum
(arrow) that probably
related to
incoordination of
esophageal peristalsis
and relaxation of the
lower esophageal
sphincter
25. ESOPHAGEAL VARICES :
The characteristic radiographic appearance
1. Serpiginous filling defects which
appear as round or oval filling
defects resembling the beads of a
rosary( dilated venous structures) (
arrowhead).
2. Changes size and appearance
with variations in intrathoracic
pressure and collapse with
esophageal peristalsis and
distension.
3. Varices related to portal
hypertension are most commonly
demonstrated in the lower third of
the esophagus.
4. In portal hypertension ;
common accompanying gastric
varices(arrow).
31. Air-contrast esophagram shows thick esophageal mucosal folds
(arrows) and an ulcer (arrowhead) due to GERD.
Single contrast esophagram shows stricture (arrow) and sliding
hiatus hernia
32. INFECTIOUS ESOPHAGITIS : Increasingly common because of
the use of steroid and cytotoxic drugs, disseminated malignancy,
and increasing incidence of acquired immunodeficiency syndrome
CANDIDA ESOPHAGITIS
Radiographic findings include
1. Abnormql esophageal motility ( dilated,
atonic esophagus ) is often an early stage
2. Irregular, nodular, plaque-like mucosal
pattern ( arrow), irregular folds(arrowhead)
with marginal serrations ( shaggy appearance )
3. Multiple ulcerations of various sizes
4. Frequently involve the entire thoracic
esophagus
38. CORROSIVE ESOPHAGITIS.
Most severe corrosive injuries are caused by alkalis
Barium study is unnecessary during acute phase.
Radiographic findings;
1. Diffuse superficial or deep ulceration
involving long portion of the distal
esophagus
2. Abnormal motility
3. Fibrotic healing results in a long
esophageal stricture ( arrow) that
extends down to the cardioesophageal
junction.
Note : barium was aspirated into left main
bronchus(green arrow)
41. Symmetric tapered benign stricture
months after radiotherapy.
Benign stricture high in the esophagus
(arrow). There is bilateral lower lobe lung
consolidation due to repeated aspiration.
45. Boerhaave syndrome:
Boerhaave's syndrome is rupture of the esophageal wall.
It is most often caused by excessive vomiting in eating
disorders such as bulimia although it may rarely occur in
extremely forceful coughing or other situations, such as
obstruction by food.
Boerhaave's syndrome is a transmural or full-thickness
perforation of the esophagus, distinct from Mallory-
Weiss syndrome, a non-transmural esophageal tear also
associated with vomiting.
These syndromes are distinct from iatrogenic perforation,
which accounts for 85-90% of cases of esophageal
rupture, typically as a complication of an endoscopic
procedure, feeding tube, or unrelated surgery.
47. Mallory-Weiss tear
A Mallory-Weiss tear results from prolonged and
forceful vomiting, coughing or convulsions.
Typically the mucous membrane at the junction of
the esophagus and the stomach develops
lacerations which bleed, evident by bright red
blood in vomitus, or bloody stools.
It may occur as a result of excessive alcohol
ingestion.
This is an acute condition which usually resolves
within 10 days without special treatment.
49. Esophageal hematoma:
These unusual lesions have been associated with
increased esophageal intraluminal pressure, most
often vomiting, instrumentation, and
anticoagulation or bleeding disorders.
Some are spontaneous.
Blunt trauma is a rare cause.
Hematomas are self-limited and almost never
progress to perforation.
Most esophageal hematomas resolve in 1-2 weeks
with conservative treatment.
53. Leiomyomas
Leiomyomas are the most common benign esophageal
neoplasm and are often large yet nonobstructive.
Gastrointestinal stromal tumors (GIST) are least common
in the esophagus.
54. A calcified esophageal mass is almost always a leiomyoma.
On the left a patient with a calcified esophageal lesion (arrows)
protrudes into azygoesophageal recess on radiograph.
61. ADVANCED STAGE
A. Large Polypoid ( often
fungating ) filling defect
(arrow) with overhanging
edge (yellow arrow)
B. Large ulcer niche (yellow
arrow) within a bulging
mass (ulcerated mass)
(arrow)
Major radiographic appearances
62. Major radiographic appearances.
Advanced stage
A. Encircling mass with
irregular luminal
narrowing (green arrow)
and shelf like margins
(black arrow)
B. Nodular thickened folds
(varicoid type) (black arrow);
Extension of the tumor
(green arrow)
63. PSEUDO-ACHALASIA caused by direct spread to the
distal esophagus from gastric carcinoma.
Radiographic findings :
1. Irregularly, narrowed
and nodular( arrowhead),
sometimes ulcerated
(arrow), lesion at distal
esophagus
2. Rapid transition
between normal and
abnormal part.
3. Dilatation of proximal
esophagus