Hepatic encephalopathy by Dr.V.B.Kasyapa.J
•Download as PPTX, PDF•
4 likes•363 views

Hepatic Encephalopathy from Harrison 19th Edition, Schiffs 11th Edition and some Internet Sources Prepared in March, 2018.

Recommended
Recommended
More Related Content
Similar to Hepatic encephalopathy by Dr.V.B.Kasyapa.J
Similar to Hepatic encephalopathy by Dr.V.B.Kasyapa.J (20)
More from Veerabhadra Kasyapa J
Recently uploaded
Recently uploaded (20)
Hepatic encephalopathy by Dr.V.B.Kasyapa.J
- 1. Hepatic Encephalopathy Dr.V.B.Kasyapa.J. II year, MD – Gen. MODERATOR: Dr.K.Venkateswarlu MD Prof., Dept. of GM.
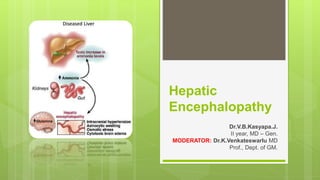
- 2. Introduction Brain dysfunction caused by liver insufficiency and/or portosystemic shunting, and manifests as a wide spectrum of neurological/ psychiatric abnormalities ranging from subclinical alterations to coma. Even with only porto-systemic anastomoses, without intrinsic liver pathology, HE is rare. 03-04-2018 13:32:472
- 4. Definitions Overt HE is the clinical manifestation of HE where changes in consciousness and motor abnormalities are observed. Minimal HE is defined as patients with completely normal neurologic examination but who have cognitive deficits in specific domains which are detected by psychometric tests. Covert HE is a new term that has been proposed to encompass minimal HE and the mildest form of overt HE. 03-04-2018 13:32:474
- 6. Little More For Understanding 03-04-2018 13:32:476
- 7. Pathogenesis (MC) culprit – Gut derived toxins (by Bacteria in colon & enterocytes) Referring Introduction, 03-04-2018 13:32:477
- 8. Introduction A broad range of neurologic & neuropsychiatric impairments seen in patients with significant underlying liver disease. Even with only porto-systemic anastomoses, without intrinsic liver pathology, HE is rare. 03-04-2018 13:32:478
- 9. Pathogenesis (MC) culprit – Gut derived toxins (by Bacteria in colon & enterocytes) Referring Introduction It seems many of the patients still have Minimal HE. There will be increased hepatic artery flow for lack of portal perfusion. But if there are any added proximal (ex: lienorenal) shunts multiple bouts of overt HE. 03-04-2018 13:32:479
- 11. Ammonia Major mediator, Correlates with Astrocyte oedema. Florid oedema seizures, coma (in Acute LF) >200µmol/L S.NH3 In Chronic LF mild oedema There will not be any ↑ICP features, because Pre existing cerebral atrophy (in Alcoholic LD) Compensatory extrusion of intracellular Myoinositol; due to ↑Glutamine (from NH3 + Glutamate) 03-04-2018 13:32:4711
- 12. GABA/Benzodiazepine System Best studied ↑sensitivity of Astrocyte (peripheral) BZD receptors & ↓susceptibility of synaptosomes for solubilisation causing ↑ GABA receptors ↑Accumulation of GABA & BZD (not to the level of coma) ↑ Neurosteroids (allopregnanolone, tetra hydro-deoxy-corticosterone) in Astrocytes Feed forward mechanism. Supported by reversal of HE by FLUMAZENIL 03-04-2018 13:32:4712
- 13. Endogenous opiates In cholestatic liver disease, Accumulation of these cause Pruritus Supported by reversal by NALOXONE 03-04-2018 13:32:4713
- 14. Amino acid imbalance ↓ Branched chain amino acids (Leu, Ilu, Val): they are mainly used up by skeletal muscle to produce Glutamate ↑Aromatic amino acids (Phe, Tyr, Try) Loss of competition for cross over at BBB. Accumulation of AAA in brain False neurotransmitters & Serotonin production with ↑intracellular Glutamine Reversal with oral BrAA 03-04-2018 13:32:4714
- 15. Inflammation/Sepsis It can be an independent Risk Factor for Encephalopathy. It can modulate the expression of overt HE Oral glutamine challenge test can be done There will be no impairment if there are no raised inflammatory markers May be due to inflammatory effect on BBB 03-04-2018 13:32:4715
- 16. Gene modulation Allelic mutation in glutaminase gene ↑Glutaminase transcriptional activity ↑Ammonia & Glutamine ↑ Risk of Overt HE 03-04-2018 13:32:4716
- 17. Colonic Microbiota There is retrospective evidence showing a difference in microbiota that resides in colon, between a normal person and a cirrhotic person. Ammoniogenic bacteria outgrows other species; reason still unknown. 03-04-2018 13:32:4717
- 18. Clinical Features Subtle findings Reversal of sleep-wake cycle (first), forgetfulness, alterations in hand writing, difficulty in driving Worst findings Asterixis, agitation, disinhibited behaviour, seizures, coma 03-04-2018 13:32:4718
- 21. Diagnosis Any change in mental status or prior performance in psychometric assays in patients with known or strongly suspected underlying cirrhosis should be considered to be HE, unless proven otherwise. 03-04-2018 13:32:4721
- 22. If we see HE with preserved liver function (ex: Ⓝ PT, INR & LFT) Suspect, 03-04-2018 13:32:4722
- 25. Modified West Havens Criteria 03-04-2018 13:32:4725
- 26. HESA (Hepatic encephalopathy Scoring Algorithm) combines clinical impressions with neuropsychological performances to characterize HE. To overcome variability in assessment of lower grades of HE. Shows early promise. 03-04-2018 13:32:4726
- 27. CHESS (Clinical HE Staging Scale) It has 9 questions Not much useful for minimal HE. 0-9 scores. Higher the score, severe the HE. 03-04-2018 13:32:4727
- 28. ISHEN (International Society for HE & Nitrogen metabolism) Mainly divided HE in to two categories Covert HE: Minimal HE + Stage 1 WHC Overt HE: Stage 2,3&4 WHC 03-04-2018 13:32:4728
- 29. Neurologic assessment Hypertonia, Hyper-reflexia, Extensor plantar reflexes, Transient decerebrate posturing, Nystagmus, Ataxic finger nose & knee heel test, Dysdiadokinesia. Signs of progressive cerebral dysfunction Dementia, Motor deficits, etc.. (MC) motor: disruption of smooth pursuit of eye movements (SPEM) 03-04-2018 13:32:4729
- 31. Asterixis Flapping tremor. Failure to actively maintain posture/ position. Postural lapse that occurs consists of series of rapid, involuntary, flexion – extension movements of wrist (Hepatic Flap). MOA: abnormal function of supraspinal motor centres. Seen in Grade II HE on WHS; also in RF, CHF, Resp.F, Frontal lobe lesions, Hypokalaemia. Other places to appreciate: Tongue protrusion, dorsiflexion of foot, fist clenching, forced eye closure. 03-04-2018 13:32:4731
- 33. Lab diagnostic tests 03-04-2018 13:32:4733
- 34. Serum Ammonia testing 03-04-2018 13:32:4734
- 35. CSF Amino acids Glutamate (in astrocytes Glutamine) 2 fold increase ↑Phe, Tyr (precursors of Dopamine, NE) Most predictable risk in AA relating to degree of neurologic deterioration CSF Alanine 03-04-2018 13:32:4735
- 36. Psychometric Tests Paper-pencil tests PHES (Psychometric HE Score)- gold standard Number connection test A,B; Serial dotting test; Digit symbol test; Line tracing test Domains: motor speed, accuracy, visual perception, visuospatial orientation, visual construction, concentration, attention & memory(to lesser extent) RBANS (Repeatable Battery for Assessment of Neuropsychological Status) Four alternative forms (A D); 20-30 min Correlates with MELD score Remarkable learning effect little useful with close intervals 03-04-2018 13:32:4736
- 38. Computer based tests: for minimal HE ICT(Inhibitory Control Test): 6 runs/2 min For deficits in attention, response inhibition. Also used in ADD, Schizophrenia, Brain injury. XY/YX space bar; XX/YY refrain >5 lure response Minimal HE (88% sensitivity) CDR(Cognitive Drug Research Test) 7 tests 5 domains (power of attention, continuity of attention, quality of episodic memory, quality of working memory, speed of memory) 03-04-2018 13:32:4738
- 39. Critical Flicker Fusion Frequency Test: 15 min Principle: Hepatic retinopathy Muller cells in retina = Astrocytes (similar changes) Changes in light frequency perception by retina 60Hz ↓0.1Hz/sec first perception of light pulses; <39Hz Minimal HE Prerequisite: binocular vision No learning effect 03-04-2018 13:32:4739
- 40. EEG To objectively quantify the degree of physiologic changes in brain & to study its correlation with other tests. In research setting; To monitor effects of therapy, portosystemic shunt insertion, surgery & OLT In clinical setting; for severely impaired Generalized slowing of background EEG activity (in other encephalopathies) ↓Amplitude of waves Triphasic waves & bursts of slow activity in theta & delta range 03-04-2018 13:32:4740
- 42. Newer ANESS (Artificial Neural Network Expert System Software) SEDACA (Short Epoch, Dominant Activity, Cluster Analysis) 03-04-2018 13:32:4742
- 46. Supportive care Nasogastric tube for delivery of Lactulose. Elective intubation (in severe HE), To prevent aspiration of Lactulose & GI bleed. NG tube feeding, After initial recovery phase of GI bleed and initial washout. 03-04-2018 13:32:4746
- 48. BrAA supplementation They are mainly used up to produce more and more glutamate. So, using BrAA supplement may cause more detriment, as per many authors. So they suggest adding, α-keto glutarate (to prevent Glutamine breakdown by enterocytes). Phenyl butyrate (to increase Glutamine excretion by kidneys). 03-04-2018 13:32:4748
- 49. Precipitating factors (MI) aspect of therapy Many patients have >2 simultaneous factors (MC) overall – Sepsis (MC) in CLD – Upper GI bleed (it is more ammoniogenic compared to other proteins d/t lack of isoleucine in RBC) Do gut lavage & catharsis If constipation or ileus present rectal lactulose Look for Hyponatremia 03-04-2018 13:32:4749
- 52. Lactulose Non absorbed disaccharide FDA, 1977 Most important drug No clear data It has become an ethical issue No difference from cheaper laxatives Need placebo controlled trials 03-04-2018 13:32:4752
- 53. Rifaximine Minimally absorbed broad spectrum antibiotic No placebo controlled trials More useful in recurrent HE & Lactulose failure? No proof in shortening the overt HE episodes MOA: it preferentially kills small bowel bacterial over growth, without having much effect on colonic microbiota It is activated by bile salts Also effective against Clostridium difficile 03-04-2018 13:32:4753
- 54. Others Neomycin, May have efficacy, but toxicity ended its use It is not towards anaerobic bacteria New found use: inhibits intestinal mucosal enzyme glutaminase Most useful in gene defects. Metronidazole, Vancomycin, Paramomycin Possibly by bacterial growth suppression Only short-term use Flumazenil ‘Awakenings’ seen in 30% of patients without ant prior BZD use 03-04-2018 13:32:4754
- 55. Old Concepts Urease immunization Colonic resection/bypass Arterialisation of Portal vein stump 03-04-2018 13:32:4755
- 56. HE with ALF Early ↑ICP uncal herniation coma, death. Arterial NH3, partial pressure of NH3,,ICP – independent outcome predictors. HE stage 4 = 80% chance of cerebral edema. On EEG subclinical epileptiform cortical activity (d/t ↑ glutamine in Astrocytes) Advanced cerebral edema: hyperventilation, systemic HTN, pupillary abnormalities, decerebrate posture,uncal herniation and death. 03-04-2018 13:32:4756
- 57. HE with ALF Lactulose best for 1,2 stage HE Elevate the bed (300), minimize pt stimulation, elective mechanical ventilation with sedation. acute hyperventilation fails to ↓number of edema attacks or onset of herniation. Arterial NH3 >200µg/dL correlates with cerebral edema. Irrevesible brain injury: ICP >20mm Hg, CPP <50mm Hg ICP monitors useful while OLT,but risk in coagulopathy 03-04-2018 13:32:4757
- 58. HE with ALF First line: IV mannitol (0.5 g/kg body wt) [↓in Renal failure & go for RRT to ensure multiple doses], if CPP <50 mm Hg (start vasopressors), phenobarbital/thopental coma, phenytoin, mild to moderate hypothermia. Corticosteroids have no role. OLT is definitve treatment. ICP rise continues for 24hrs after OLT monitor till pt is awake. If primary graft failure/ delayed graft function continue support till hepatic recovery/retransplantation. 03-04-2018 13:32:4758
- 59. Liver transplantation When medical therapy fails Priority is given now according MELD score, which doesn’t include HE Even with severe HE, patient has to wait till he has the needed MELD score. Modified MELD (includes Hyponatremia) may be more useful In recurrent HE muscle mass depletes rapidly patient becomes less fit for survival after LT 03-04-2018 13:32:4759
- 60. Future Concepts Making PHES gold standard ↑Psychiatric test usage, worldwide. Placebo-controlled trials are largely going on. In pursuit of better systems for detection & quantification of Minimal HE. Overt HE is not completely reversible, as previously thought. Rules to earlier Liver Transplantation. 03-04-2018 13:32:4760