Acute Bronchitis Causes Symptoms Diagnosis Treatment
•
9 likes•2,922 views

Disorders of Respiratory system and Nursing Care

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Acute Bronchitis Causes Symptoms Diagnosis Treatment
Similar to Acute Bronchitis Causes Symptoms Diagnosis Treatment (20)
More from V4Veeru25
More from V4Veeru25 (20)
Recently uploaded
Recently uploaded (20)
Acute Bronchitis Causes Symptoms Diagnosis Treatment
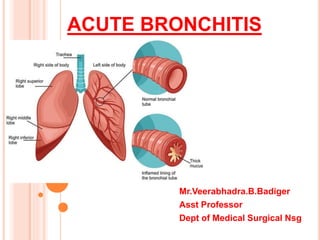
- 1. ACUTE BRONCHITIS Mr.Veerabhadra.B.Badiger Asst Professor Dept of Medical Surgical Nsg
- 2. ACUTE BRONCHITIS. Acute bronchitis is an inflammation of the bronchi in the lower respiratory tract. The inflammation also involves the mucous membrane of the trachea. Acute bronchitis typically lasts less than 10 days, but the coughing can continue for several weeks.
- 3. CAUSES OF ACUTE BRONCHITIS: Viral infection (85 to 95 percent) Bactertial infection (Mycoplasma pneumoniae , Chlamydia pneumoniae, and Bordetella pertussis ). Smoking Elderly people being very susceptible; Malnutrition Air pollutions Poor ventilation Overcrowding Occupations exposures whereby irritant particles are inhaled,
- 4. RISK FACTORS Factors that increase your risk of acute bronchitis include: Cigarette smoke , including secondhand smoke Weakened immune system Gastric reflux Frequent exposure to irritants, including dust or chemical fumes Lack of vaccinations for the flu, pneumonia, and whooping cough Age older than 50 year
- 5. PATHOPHYSIOLOGY Due to etiology Inflammation of mucous membrane of the trachea and bronchi , later it become congested and swollen But soon becomes opaque, and finally muco- purulent. swelling of the mucous glands & smaller bronchial tubes are dilated. Mucosa becomes infiltrated with leukocytes causes narrowing of bronchi.
- 6. CLINICAL MANISFESATION Common cold Throat is dry and rough , sore throat Voice is hoarse. Fever (100°F to 100.4°F (37.7°C to 38°C) Cough with expectoration Dull pain in the chest. Wheezing Malaise Generalised weakness. Coated tongue Headache.
- 7. DIAGNOSTIC STUDIES History collection Physical examination : Chest auscultation ( Rhonchi sounds). Chest x-ray Sputum analysis. Arterial blood gas studies.. Spirometry Pulmonary function test CT / MRI Chest
- 9. MANAGEMENT Symptomatic Management NSAID’s (Analgesics) & Anti-inflammatory :Ibuprofen and Naproxen To relieve pain , reduce fever& inflammation. Cough suppressants. Corticosteroids: prednisolone. To control inflmmation. Antibiotics: Based on causative agent.(Amoxicillin, Oxytetracycline or Doxycycline.) Bronchodilators. Ipratropium , Theophylline
- 10. Oxygen Therapy Nebulization. (Albuterol) Steam inhalation. Nutritional diet. Surgery: Lung transplant is optional in case lung is severe damaged
- 11. NURSING DIAGNOSIS Impaired gas exchange related to obstructed airways. Ineffective breathing pattern related to excess mucus production. Activity intolerance related to breathlessness.
- 12. NURSING CARE. Check Respiratory status of the patient. Provide comfortable bed & position. Monitor vital signs & spo2 Encourage ambulation, coughing, and deep breathing. adequate fluid intake to liquefy secretions. Encourage rest, avoidance of bronchial irritant. Administer oxygen & medications as ordered.
- 14. CHRONIC BRONCHITIS A repeated inflammation of the mucous membrane of the trachea and bronchi, that causes continuous irritation & swelling of airways. Causes Pneumonia Organic heart disease Rheumatism Syphilis Tuberculosis Chronic alcoholism Chemical irritants.
- 15. CLINICAL MANIFESTATION Cough, the expectoration Difficulty in breathing, causing exhaustion Fever with chills Tachypnoea Tachycardia Tight chest
- 16. DIAGNOSTIC STUDIES History collection Physical examination. Pulmonary function test Chest x-ray Computed tomography of chest Arterial blood gas studies. Sputum studies Complete blood count: WBC count Blood culture.
- 17. MANAGEMENT Same as acute bronchitis…… Additionally Oxygen therapy Anti-inflammatory agents: Steroids. Antibiotics: Based on agents Antipyretics. Branchodilator. Nebulization Steam inhalation.
- 18. NURSING MANAGEMENT Provide comfortable bed & position Assess vital signs ( Spo2, Pao2, Paco2) Administer oxygen if required. Provide well balanced diet Health education on personal hygiene , medication ,Follow-up care. Deep breathing & coughing exercises. Steam inhalation