1. MARCH JOGC MARS 2011 l 235
Retrospective Review of Prenatal Care and
Perinatal Outcomes in a Group of Uninsured
Pregnant Women
Catherine Jarvis, MD,1,2
Marie Munoz, MD,2,3
Lisa Graves, MD,4
Randolph Stephenson, PhD,1
Vinita D’Souza, MSc,1
Vania Jimenez, MD2,3
1
Herzl Family Practice Centre, Jewish General Hospital, Montreal QC
2
Department of Family Medicine, McGill University, Montreal QC
3
Centre de Recherche et de Formation, Centre de santé et de sociaux de la Montagne, Montreal QC
4
Northern Ontario School of Medicine, Sudbury ON
OBSTETRICS
Key Words: Medically uninsured, pregnancy, prenatal care,
undocumented, precarious status, Kotelchuck Index
Competing Interests: None declared.
Received on June 1, 2010
Accepted on October 13, 2010
Abstract
Objective: To assess the adequacy of prenatal care and perinatal
outcomes for uninsured pregnant women at two primary care
centres in Canada.
Methods: We conducted a retrospective case comparison study of
uninsured women presenting for prenatal care between 2004
and 2007 (n = 71). Control subjects (n = 72) were chosen from
provincially insured women presenting for prenatal care during
the same period. A modified Kotelchuck Index was used to
assess adequacy of care. Frequency of routine prenatal testing
(blood tests, ultrasound, cervical swabs, Pap testing, and
genetic screening) was compared. Perinatal outcomes assessed
included gestational age and birth weight.
Results: Uninsured pregnant women presented for initial care 13.6
weeks later than insured women (at 25.6 weeks vs. 12.0 weeks,
P < 0.001). Uninsured women had fewer blood tests (93.7% vs.
100%, P = 0.045), ultrasound screenings (82.5% vs. 98.4%,
P = 0.003), cervical swabs (69.8% vs. 85.2%, P = 0.04), Pap
tests (38.1% vs. 75.4%, P < 0.001), genetic screenings (12.7%
vs. 44.3%, P < 0.001), and visits with health care providers (6.6
vs. 10.7, P = 0.05). Using a modified Kotelchuck Adequacy of
Prenatal Care Utilization Index, uninsured women were more
likely to be categorized as receiving “inadequate care” (uninsured
61.9% vs. insured 11.7%, P < 0.001).
Conclusion: This study begins to document the care of uninsured
pregnant women in Canada. Women in this category presented
late for prenatal care, were less likely to have adequate
screening tests, and were more likely to receive “inadequate
care” as defined by the modified Kotelchuck Index. This
information may be valuable in helping to plan programs
to improve access to timely and adequate medical care for
uninsured pregnant women.
Résumé
Objectif : Évaluer la suffisance des soins prénatals et des issues
périnatales pour ce qui est des femmes enceintes non assurées
au sein de deux centres de soins primaires au Canada.
Méthodes : Nous avons mené une étude rétrospective de
comparaison de cas de femmes non assurées ayant cherché
à obtenir des soins prénatals entre 2004 et 2007 (n = 71). Les
témoins (n = 72) ont été choisis parmi des femmes bénéficiant
d’une assurance provinciale qui cherchaient à obtenir des soins
prénatals au cours de la même période. Un indice de Kotelchuck
modifié a été utilisé pour évaluer la suffisance des soins. La
fréquence du dépistage prénatal régulier (analyses sanguines,
échographie, frottis cervicaux, tests de Pap et dépistage
génétique) a été comparée. Parmi les issues périnatales
évaluées, on trouvait l’âge gestationnel et le poids de naissance.
Résultats : Les femmes enceintes non assurées cherchaient
à obtenir des soins initiaux 13,6 semaines plus tard que
les femmes assurées (à 25,6 semaines, par comp. avec
12,0 semaines, P < 0,001). Les femmes enceintes non assurées
bénéficiaient de moins d’analyses sanguines (93,7 %, par comp.
avec 100 %, P = 0,045), de dépistages échographiques (82,5 %,
par comp. avec 98,4 %, P = 0,003), de frottis cervicaux (69,8 %,
par comp. avec 85,2 %, P = 0,04), de tests de Pap (38,1 %,
par comp. avec 75,4 %, P < 0,001), de dépistages génétiques
(12,7 %, par comp. avec 44,3 %, P < 0,001) et de consultations
auprès de fournisseurs de soins (6,6, par comp. avec 10,7,
P = 0,05). En ayant recours à un indice Kotelchuck Adequacy
of Prenatal Care Utilization modifié, nous avons constaté que
les femmes non assurées étaient plus susceptibles d’être
catégorisées comme recevant des « soins inadéquats » (61,9 %
des femmes non assurées, par comp. avec 11,7 % des femmes
assurées, P < 0,001).
Conclusion : Cette étude commence à documenter les soins offerts
aux femmes enceintes non assurées au Canada. Les femmes
2. 236 l MARCH JOGC MARS 2011
OBSTETRICS
de cette catégorie cherchaient tard à obtenir des soins prénatals,
étaient moins susceptibles de bénéficier de tests de dépistage
adéquats et étaient plus susceptibles de recevoir des « soins
inadéquats », tels que définis par l’indice de Kotelchuck modifié.
Cette information pourrait s’avérer utile dans la planification
de programmes visant à améliorer l’offre de soins médicaux
adéquats et offerts en temps opportun aux femmes enceintes
non assurées.
J Obstet Gynaecol Can 2011;33(3):235–243
INTRODUCTION
In 1990, the World Summit for Children adopted the
specific goal of helping all pregnant women access
prenatalcare,basedonevidencethatantenatalcareimproves
maternal and perinatal health.1,2
Canada provides access
to prenatal care and delivery services through a system
of universal health care coverage which is administered
through provincial, territorial, or federal health insurance
plans.3
Although Canada’s health care system is universal in
principle, in practice there are people living in Canada who
are not eligible for government insurance.4
These people
include not only undocumented (illegal) immigrants, but
also those who have precarious status such as tourists,
visitors, foreign students, undocumented asylum seekers,
and persons who are between different status types.
Pregnant women constitute a particularly vulnerable
subgroup of the uninsured because their status in Canada
limitsaccesstoprenatalanddeliveryservicesassociatedwith
healthy maternal and child birth outcomes.1,2
Publications
addressing this issue are notably lacking, which may reflect
the challenges of studying this population. The uninsured
are difficult to study for reasons that include their reluctance
to be identified, the fact that they are often transient and
mobile, and the various institutional barriers to care that
they face.5
European data suggest that uninsured prenatal patients
are more likely to receive inadequate prenatal care and
are at increased risk of perinatal death.6,7
A study in West
Virginia showed a decrease in the fetal death rate after the
introduction of a program to provide free prenatal care
to the uninsured.8
Several other studies have also shown
a link between inadequate, late, or no prenatal care and an
increased risk of preterm delivery.9–11
In Canada, Caulford
and Vali observed that 60% of pregnant uninsured
immigrant women seen in a Toronto clinic had deficiencies
in prenatal care.12
The objective of this study was to document the adequacy
of prenatal care and perinatal outcomes for all uninsured
pregnant women seen at two primary care centres in
Montreal.
METHODS
Given the inherent difficulties in studying the uninsured,
we chose to use a retrospective approach to data collection
for this study, and used a convenience sample representing
only uninsured women who presented to a family medicine
obstetric group for prenatal care.
The study was conducted at two family practice centres in
Montreal, the Herzl Family Practice Centre and the Centre
Local de Services Communautaires Cote des Neiges. Both
sites share the same family medicine obstetric call group
and use the same hospital, the Jewish General Hospital,
for deliveries. The two centres are located across the
street from each other in a multiethnic neighbourhood.
Uninsured women had been noted to use these clinics for
prenatal care. Although the study sites are geographically
linked, the CLSC CDN hosts a government-funded site of
referral for refugee claimants and therefore has funding and
resources that are not available at the Herzl Family Practice
Centre. At the time of the study, these resources included
an obstetric team, social services specifically available to
aid in issues of status, and financial assistance that could
be organized on an ad hoc basis at the discretion of the
medical providers. Although some uninsured patients
were able to receive financial assistance for tests and visits
at this site, it is important to note that prenatal services
were never advertised as “free.” Additionally, the intent of
these services was never to reach the uninsured population
directly, but rather to provide support for immigrants in
the process of status regularization. We chose to study the
two sites together despite the differences between them.
This approach allowed us to capture a larger sample and
give a broader overview of the reality of prenatal care for
this population.
A retrospective chart audit was carried out using the medical
databases at each site. The primary goal of the study was
to compare prenatal care between insured and uninsured
women. An estimate of the total number of women
presenting for prenatal care at both centres between 2004
and 2007 was made using both the databases and monthly
ABBREVIATIONS
APNCU Adequacy of Prenatal Care Utilization Index
CLSC CDN Centre Local de Services Communautaires
Cote des Neiges
STI sexually transmitted infection
3. MARCH JOGC MARS 2011 l 237
Retrospective Review of Prenatal Care and Perinatal Outcomes in a Group of Uninsured Pregnant Women
obstetric rosters (n = 1523). We identified the medical
records of all pregnant women during this period who did
not have a valid provincial medical insurance card at initial
presentation. These records were carefully reviewed and a
cohort was formed from all women identified as having
no insurance at initial presentation (n = 71). Women
were excluded from this cohort if they had provincial
insurance coverage, private insurance, or coverage through
the Interim Federal Health Program (refugee claimants).
A second cohort was chosen randomly from provincially
insured women presenting for prenatal care during the
same period (n = 72). Patients lost to follow-up in either
group were excluded from data analysis.
A chart audit form was developed to collect basic
demographic information, information on legal status
in Canada (when available), insurance status, number
of prenatal visits, routine prenatal investigations, and
basic perinatal outcomes. Routine prenatal investigations
assessed included blood tests (complete blood count,
blood type, rubella, hepatitis B surface antigen, syphilis
serology, HIV testing), obstetric ultrasound, cervical swab
for STI, Pap testing, and genetic screening (amniocentesis
or first trimester genetic screening). Perinatal measures
assessed included route of delivery, use of epidural
analgesia, induction of labour, gestational age at birth, and
birth weight.
The Kotelchuck Index, also called the Adequacy of Prenatal
Care Utilization Index, was used to assess adequacy of
prenatal care.13
This index characterizes the adequacy of
prenatal care utilization by assessing two independent
and distinctive dimensions, namely adequacy of initiation
of care and adequacy of received services. “Adequacy of
initiation of care” assesses the timing of the first prenatal
visit. All women arriving after 21 weeks of gestation are
categorized as having received inadequate care. “Adequacy
of received services” measures the number of actual visits
compared to the number of expected visits based on
gestational age at presentation and delivery, thus controlling
for gestational age at arrival and delivery. The Kotelchuck
Index of Received Services defines adequate care as having
had at least 80% of expected visits.
The APNCU was modified with permission to reflect
local prenatal care standards (Milton Kotelchuck, personal
communication, June 24, 2009). The Kotelchuck Index is
based on the recommendations for prenatal visits issued by
the American College of Obstetricians and Gynecologists.
The Society of Obstetricians and Gynaecologists of Canada
has issued basic guidelines regarding a minimum number
of prenatal visits, but has not recommended a schedule
of prenatal visits.14
Therefore, the authors modified the
Kotelchuck Index to reflect the Canadian practice of
offering 12 prenatal visits rather than the 13 currently
recommended by the American College of Obstetricians
and Gynecologists. Our practice has been to initiate care
before 13 weeks’ gestation and to see patients monthly
from 12 to 32 weeks, biweekly from 32 to 36 weeks, and
weekly from 36 weeks to delivery. We have termed this
modified index the APNCU-Montreal.
All statistical analyses were performed with SPSS version
16 (SPSS Inc., Chicago IL). Two group t tests were used to
compare means between insured and uninsured women. A
chi-square test was used to examine two-way associations
between categorical variables. P values were considered
significant if < 0.05.
A post hoc power analysis was completed.15
The actual
power computed from the effect size, level of statistical
significance, and size of both sample groups varied from
0.99 to 1.00.
Ethics approval for the study was provided by the Research
Ethics Committee, Jewish General Hospital, and the
Comité d´éthique de la recherche du Centre de santé et de
services sociaux de la Montagne.
RESULTS
Uninsured women represented 4.7% (71/1523) of all
women followed for prenatal care at the study centres.
Eight of the uninsured women (11%) were lost to follow-
up because they did not complete prenatal care at the study
centres. Eleven insured women (15%) were lost to follow-
up and two additional charts had incomplete data.
Ninety-six percent of uninsured women in our study had
precarious status in Canada (68/71). Only three of the
uninsured women (4%) were Canadian citizens who had
let their provincial health insurance lapse. More than half
of the uninsured women in our study were undocumented
or had no official status in Canada (41/72, 57.7%). Seven
of the uninsured women (9.9%) had legal but temporary
status in Canada (visitors or students). At least 28% (20/71)
of the women in our study had recently tried to regularize,
or were currently in the process of regularizing, their status.
These women included seven refugee claimants whose
claims had been refused, five asylum seekers who had not
yet made a formal application, and eight women awaiting
sponsorship (Table 1).
There were no significant differences between uninsured
and insured women in mean age (28.6 vs. 29.2, P = 0.478),
4. 238 l MARCH JOGC MARS 2011
OBSTETRICS
gravidity (2.4 vs. 2.4, P = 0.670), or parity (0.9 vs. 0.8,
P = 0.203). Uninsured women had fewer prenatal visits than
insured women (6.6 vs. 10.7, P = 0.05). Uninsured women
presented later in their pregnancy for a first prenatal visit
than the control group (25.6 vs. 12.0 weeks, P < 0.001),
thereby presenting for initial care on average 13.6 weeks
later than insured women (Table 2). The uninsured had
fewer routine prenatal screening tests, including screening
blood tests (93.7% vs. 100%, P = 0.045), ultrasound
(82.5% vs. 98.4%, P = 0.003), STI screening (69.8% vs.
85.2%, P = 0.04), Pap tests (38.1% vs. 75.4%, P < 0.001),
and genetic testing (12.7% vs. 44.3%, P < 0.001). There
was no difference between the groups in the number of
women who had a physical examination (cardiovascular,
respiratory, and gynaecologic examination) as part of
routine prenatal care (46.1% vs. 53.9%, P = 0.183). There
were no significant differences between the groups in the
route of delivery (vaginal delivery 71.4% vs. 69.5%, P =
0.815), use of epidural analgesia (71.4% vs. 73.3%, P =
0.813), and rate of induction of labour (25.4% vs. 20%,
P = 0.476). There were no significant differences in mean
gestational age at delivery (39.0 vs. 39.2 weeks, P = 0.289),
in mean infant birth weight (3379 g vs. 3387 g, P = 0.551)
(Table 2), or in attendance at a postpartum visit (71.4% vs.
83.6%, P = 0.105).
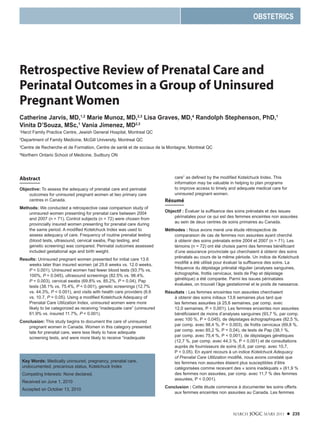
According to the APNCU-Montreal, the majority of
uninsured women were categorized as having inadequate
prenatal care utilization (61.9% vs. 11.7%, P < 0.001)
(Figure 1). There were also significant differences in the
adequacy of received services between uninsured and
insured women (inadequate services 6.3% and 1.7%
respectively, P = 0.04) (Figure 2).
A site comparison of uninsured women was carried out to
look for differences between the two centres in number of
visits and frequency of prenatal tests (Table 3). Women at
the CLSC CDN began care earlier than those at the Herzl
Centre (18.9 vs. 25.6 weeks, P = 0.012) and had a greater
total number of prenatal visits (8.3 vs. 4.7, P = 0.001).
The uninsured women who received care at the CLSC
CDN were also more likely than those who received care
at the Herzl Centre to have had swabs for STI (82.1% vs.
51.2%, P = 0.008) and Pap testing (50.0% vs. 25.6%, P =
0.035). There were no differences in the respective rates of
prenatal screening blood tests (92.9% vs. 83.7%, P = 0.26),
ultrasound (82.1% vs. 74.4%, P = 0.45), or early genetic
screening (10.7% vs. 14.0%, P = 0.45).
Ten uninsured women in the study became insured during
the course of pregnancy follow-up (10/71, 14%). All
of these women attended the CLSC CDN, which had
resources in place to assist women in regularizing their
status. Subanalysis of this group of women compared
with the uninsured women at the CLSC CDN showed
no differences in adequacy of prenatal care utilization,
adequacy of received services, or access to routine
prenatal tests.
DISCUSSION
Most uninsured women in our study (96%) had precarious
status in Canada. The uninsured included both women
with legal but temporary status in Canada and women
who were undocumented (Table 1). For these uninsured
women, access to care within a system with publicly funded
universal health insurance poses several challenges. Other
Table 1. Legal status and insurance coverage of study population
Legal status
Immigration
category
Governmental
insurance Uninsured n (%) Insured n (%)
Permanent Citizen or landed
immigrant
Medicare 3 (4.2) 72 (100)
Precarious Temporary Visitor or tourist None 5 (7)
(legal) Foreign student 2 (2.8)
Awaiting
sponsorship
8 (11.3)
“Illegal” Undocumented
immigrants
41 (57.7)
Asylum seekers
who have not yet
filed a claim
5 (7)
Refused refugee
claimants
7 (9.8)
5. MARCH JOGC MARS 2011 l 239
Retrospective Review of Prenatal Care and Perinatal Outcomes in a Group of Uninsured Pregnant Women
Canadian studies have attempted to document the barriers
to care for the uninsured.16,17
These challenges include
lack of familiarity with the medical system, inability to
find service providers who will care for them, difficulty
accessing services because of status, delayed seeking
of care, lack of proximity to services, wait lists, fear of
being reported, and the financial constraints of paying for
services out of pocket.
Uninsured pregnant women at the two centres presented
late for prenatal care, on average only beginning care
during the 25th week of gestation. These results are similar
to those documented by Caulford and Vali in Toronto.12
Arriving late for care may result in serious consequences
for both women and their babies. Late arrival means lost
screening opportunities, including genetic screening and
ultrasound screening, as well as missed opportunities for
health promotion including advice about nutrition and folic
acid intake.
Arriving late for care is an important marker in the
Kotelchuck APNCU. We documented a significant
difference between the insured and uninsured with regard
to the modified Kotelchuck Index (APNCU-Montreal)
Table 2. Prenatal care provided to insured versus uninsured women
Insured (n = 61) Uninsured (n = 63) t 2
(df = 1) P
Demographics, mean (SD)
Maternal age years 29.2 (5.9) 28.6 (5.5) −0.60* NS
Gravidity 2.4 (1.4) 2.4 (1.4) 0.12* NS
Parity 0.8 (0.9) 0.9 (1.1) 0.01* NS
Prenatal visits
Gestational age at first
visit, weeks, mean (SD)
12.0 (5.7) 25.6 (11.1) 7.27* < 0.001
Total number of prenatal
visits, mean (SD)
10.7 (3.0) 6.6 (3.4) 7.16* 0.05
Physical examination, % 53.9 46.1 1.8 NS
Prenatal tests, %
Initial screening blood
test
100.0 93.7 14 0.045
Swabs for STIs 85.2 69.8 4.2 0.04
Pap 75.4 38.1 17.6 < 0.001
Ultrasound 98.4 82.5 8.9 0.003
Early genetic screening 44.3 12.7 15.2 < 0.001
Route of delivery, %
Vaginal birth† 69.5 71.4 0.06 NS
Caesarean section† 30.5 28.6 0.06 NS
Delivery interventions, %
Epidural use‡ 73.3 71.4 0.06 NS
Induction‡ 20.0 25.4 0.51 NS
Postpartum care, %
Postpartum visit 83.6 71.4 2.62 NS
Indicators of baby’s
well-being
Gestational age at birth,
weeks, mean (SD)
39.2 (1.4) 39.0 (1.8) −0.68§ NS
Baby’s weight at birth, g
mean (SD)
3387 (510) 3379 (550) −0.09* NS
SD: standard deviation; NS: not statistically significant; df: degree of freedom
*df = 1, n = 122
†n = 59 for insured women
‡n = 60 for insured women
§df = 1, n = 121
6. 240 l MARCH JOGC MARS 2011
OBSTETRICS
(Figure 1). This is largely due to the fact that uninsured
women presented late for prenatal care. Other investigators
have shown an association between inadequate prenatal
care, as defined by the Kotelchuck Index, and increased
risk of preterm delivery9
and low birth weight,10
both
of which are major risk factors for neonatal morbidity
and mortality. Although this study did not show any
differences in the basic perinatal outcomes of gestational
age and birth weight, the study sample does not adequately
represent all uninsured women. Lu et al. showed that
undocumented women with no prenatal care were nearly
four times more likely to deliver low birth weight infants
and over seven times more likely to deliver premature
infants than undocumented women who received prenatal
care.11
Notably unrepresented in our study sample were
uninsured women who received care from midwives or
obstetricians, and those who received no prenatal care at all.
This limitation of the sample may explain why this study
failed to reproduce the results of other studies which have
documented an association between inadequate prenatal
care and preterm delivery or low birth weight. In addition
to this selection bias, our sample size was small and did not
have the statistical power to evaluate rare events such as
neonatal morbidity or mortality accurately.
Women who were uninsured came for fewer total visits
than insured women. This finding could reflect the fact
that uninsured women began care late in their pregnancy
and therefore had fewer total visits. To control for this,
the Kotelchuck Index of Received Services was used.
Even when controlling for late onset of care using this
index, uninsured women had significantly fewer visits
than is recommended. As seen in Figure 2, nearly 40% of
uninsured women were categorized as receiving inadequate
or intermediate care, meaning that they attended fewer
than 80% of the recommended visits. It is unclear why
uninsured women attend fewer visits, but the financial cost
of such visits is likely to play a role. A site comparison
showed that uninsured women at the CLSC CDN had
more visits and were more often categorized as having had
Figure 1. Distribution of adequacy of prenatal care utilization
Note: See Kotelchuck13
for explanation of the Adequacy of Prenatal Care Utilization Index.
Figure 2. Distribution of adequacy of received services
Note: See Kotelchuck13
for explanation of the Adequacy of Received Services Index
11.7%
61.9%
13.3%
12.7%
55.0%
20.6%
20.0%
4.8%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Insured (n =60)
Uninsured (n =63)
Inadequate
Intermediate
Adequate
Adequateplus
χ2 = 36.3, P = 0.001
1.7%
6.3%
15.0%
33.3%
58.3%
44.4%
25.0%
15.9%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Insured (n =60)
Uninsured (n =63)
Inadequate
Intermediate
Adequate
Adequateplus
χ2 = 8.3, P = 0.04
7. MARCH JOGC MARS 2011 l 241
Retrospective Review of Prenatal Care and Perinatal Outcomes in a Group of Uninsured Pregnant Women
an adequate number of visits according to the Adequacy
of Received Services Index. This suggests that there may
be an association between increased attendance at prenatal
visits and services provided free of charge. Although this
study was not formally designed to evaluate the differences
between the two sites, these noted differences do suggest
that further study to compare the models of care delivery
would be important when evaluating adequacy of
prenatal care.
Uninsured women had fewer routine prenatal screening
tests, including blood tests, ultrasound examinations,
swabs for STI, Pap tests, and genetic screening than
women with insurance (Table 2). This difference in rates
of screening may in part be due to the financial cost of
testing, which would be borne directly by uninsured
patients. This conclusion is supported by the observation
that when patients had access to the financial support
available at the CLSC CDN site for screening tests, more
women had such testing done (Table 3). Although it may
appear that providing financial assistance for screening
tests is likely to increase rates of screening, the issue is
more complicated than finances alone. For example, the
differences observed between the uninsured and the
insured with regard to genetic screening tests may be due to
the fact that undocumented women arrived later for care,
thereby missing the opportunity to have genetic screening
tests that are usually done before 18 weeks. Further study
will be required to better understand all the barriers that
prevent uninsured women from undergoing recommended
prenatal screening tests. The differences in specific rates of
prenatal testing by the uninsured are of interest. Uninsured
women were more likely to have had blood and ultrasound
testing than to have had swabs for STI, Pap testing, or early
genetic screening (Table 2). This may indicate that when
women have to pay for services they must balance the cost
of testing against the perceived value of the test. Women
or their care providers may consider blood and ultrasound
testing to be more important than the other investigations.
Rates of STI screening and Pap tests were significantly
higher at the CLSC CDN, where financial support was
provided for testing (Table 3). This suggests that financial
costs play a role in screening rates.
The potential risk to mother and fetus of failing to have
routine prenatal testing is difficult to quantify. Several
studies in the United States have examined the public health
implicationsof notfundingprenatalcareforundocumented
immigrants.11,18,19
One study in California concluded that
eliminating public funding for STI screening of pregnant
undocumented migrants would lead to increased STI-
related morbidity and costs.19
Providing adequate prenatal
screening has the potential to decrease health care costs
related to STIs, preterm births, and poor birth outcomes.
All the women who became insured during the course of
prenatal follow-up were followed at the CLSC CDN site.
There were no differences in the care received at this site
by those who became insured and by those who remained
uninsured. It is difficult to interpret this lack of difference.
It may indicate that the two groups were ultimately
no different in their access to prenatal care resources,
or, because uninsured women tended to arrive late for
prenatal care, it may suggest that becoming insured late in
pregnancy has no effect on the adequacy of care. A more
comprehensive study to evaluate the effects of a change of
insurance status on prenatal care utilization and outcomes
would be important.
There are several limitations to our study. First, there are
inherent difficulties in studying this population as the
uninsured in Canada are frequently undocumented and
do not necessarily want to identify themselves. Therefore,
the study sample reflects only a self-selected group of
uninsured pregnant women who succeeded in accessing
prenatal care at primary care centres. This study used a
sample that does not represent any uninsured women
with no prenatal care. Given that women with no care
tend to have worse outcomes,11
it is likely that our results
significantly under-represent the magnitude of the
problem. Additionally, since one of the study centres was
able to provide financial assistance to patients, this may
have negated some of the effect that lack of insurance has
on health service utilization and access to prenatal testing.
In this retrospective chart review, it was not possible to
gather important sociodemographic information such as
social status, education level, or income. Indeed, education
and poverty have been linked to late initiation of prenatal
care.20
This study could not assess these and other important
confounding variables including behavioural factors and
the healthy migrant effect, which may protect pregnant
migrant women from poor perinatal outcomes.21
Despite these limitations, some important differences
were detected in the prenatal care of uninsured women
compared to those with insurance. It would therefore
seem prudent to undertake a larger prospective multicentre
study with enough statistical power to detect differences in
obstetric outcomes, so as to better understand the health
consequences and costs to the medical system of caring
for uninsured pregnant women. It would seem equally
important to consider how better to provide adequate and
timely prenatal care to uninsured women and their unborn
children. We agree with Rousseau et al. that research
8. 242 l MARCH JOGC MARS 2011
OBSTETRICS
Table 3. Site comparison of prenatal care provision for uninsured women
Herzl
(n = 43)
CLSC CDN
(n = 28) t
2
(df = 1) P
Demographics
Maternal age (SD) 29.5 (5.25) 27.5 (5.76) −1.48* NS
Gravidity (SD) 2.3 (1.50) 2.7 (1.63) 1.09* NS
Parity (SD) 0.7 (1.10) 1.1 (1.24) 1.50* NS
Prenatal visits
Gestational age at first visit
in weeks (SD)
25.6 (10.8) 18.9 (10.4) −2.59* 0.012
Total number of prenatal
visits (SD)
4.7 (3.24) 8.3 (2.88) 4.66* 0.001
Adequate received services 45.9% 80.8% 15.28† 0.002
Prenatal tests
Initial screening blood test 83.7% 92.9% 1.28 NS
Swabs for sexually
transmitted infections
51.2% 82.1% 7.01 0.008
Pap testing 25.6% 50.0% 4.43 0.035
Ultrasound 74.4% 82.1% 0.58 NS
Early genetic screening 14.0% 10.7% 1.61‡ NS
SD: standard deviation; NS: not statistically significant; df: degree of freedom
*df = 1, n = 69
†df = 3
‡df = 2
examining the public health consequences and costs
associated with health care for the uninsured in Canada
should be a priority.17
The American College of Obstetricians and Gynecologists
recently issued a committee opinion statement calling for
elimination of the disparities in health status and health
care access among women, including undocumented
immigrants. “Immigrant women living within our borders
should have the same access to basic preventive health
care as U.S. citizens without regard to their country of
origin or documentation of their status.”22
The committee
noted that many of the children born to undocumented
migrants become citizens of the United States. Similarly,
undocumented migrants who come to Canada often
remain here, and most of the babies born to these women
become Canadian citizens. It is therefore in the interests
of the health care system to consider how we can provide
adequate prenatal care to these women.
CONCLUSION
The uninsured women in our study presented late for
prenatal care and were less likely to receive both routine
prenatal screening tests and adequate prenatal care. This
information is important in helping to plan for programs
to improve access to timely and adequate medical care for
uninsured pregnant women in Canada.
ACKNOWLEDGEMENTS
Herzl Research and Development Funds provided the
support of a research assistant for this study.
Dr Marissa Zampini aided with data collection.
Dr Roland Grad of Herzl Family Practice Centre, Jewish
General Hospital, and Dr Christian Holcroft of Centre
for Clinical Epidemiology and Community Studies,
Jewish General Hospital assisted with manuscript review
and revision.
REFERENCES
1. UNICEF. Plan of action for implementing the World Declaration on the
Survival, Protection and Development of Children in the 1990s. Available
at: http://www.unicef.org/wsc/plan.htm. Accessed December 21, 2010.
2. WHO, UNICEF. Antenatal care in developing countries: promises,
achievements and missed opportunities: an analysis of trends, levels and
differentials, 1990–2001. Available at: http://www.childinfo.org/files/
antenatal_care.pdf. Accessed April 21, 2010.
9. MARCH JOGC MARS 2011 l 243
Retrospective Review of Prenatal Care and Perinatal Outcomes in a Group of Uninsured Pregnant Women
3. Health Canada. Canada Health Act Annual Report 2007–2008. Available
at: http://www.hc-sc.gc.ca/hcs-sss/pubs/cha-lcs/2008-cha-lcs-ar-ra/
index-eng.php. Accessed February 14, 2010.
4. Munoz M, Chirgwin J. Les immigrants et les demandeurs d’asile: nouveaux
defis [Immigrants and asylum seekers: new challenges]. Le Médecin du
Québec 2007;42(2):33–43.
5. Magalhaes L, Carrasco C, Gastaldo D. Undocumented migrants in
Canada: a scope literature review on health, access to services, and working
conditions. J Immigr Minor Health 2010;12:132–51.
6. Barlow P, Haumont D, Degueldre M. Devenir Obstétrical et Périnatal
Des Patientes Sans Couverture Sociale [Obstetrical and perinatal
outcomes in patients not covered by medical insurance]. Rev Med Brux
1994;15:366–70.
7. Delvaux T, Buekens P, Godin I, Boutsen M. Barriers to prenatal care in
Europe. Am J Prev Med 2001;21:52–9.
8. Foster D, Guzick D, Pulliam R. The impact of prenatal care on fetal and
neonatal death rates for uninsured patients: a “natural experiment” in West
Virginia. Obstet Gynecol 1992;79:40–5.
9. Wilson A, Munson D, Schubot D, Leonardson G, Stevens D. Does
prenatal care decrease the incidence and cost of neonatal intensive care
admissions?Am J Perinatol 1992;281–4.
10. Krueger P, Scholl T. Adequacy of prenatal care and pregnancy outcome.
J Am Osteopath Assoc 2000;100:485–92.
11. Lu M, Lin Y, Prietto N, Garite T. Elimination of public funding of
prenatal care for undocumented immigrants in California: a cost/benefit
analysis. Am J Obstet Gynecol 2000;182:233–9.
12. Caulford P, Vali Y. Providing health care to medically uninsured
immigrants and refugees. CMAJ 2006;174:1253–4.
13. Kotelchuck M. An evaluation of the Kessner Adequacy of Prenatal Care
Index and a proposed Adequacy of Prenatal Care Utilization Index.
Am J Public Health 1994;84:1414–20.
14. Farrell S, Roye C, Crane J, Davis D, Heywood M, Lalonde A, et al.; SOGC
Committee on Wait Times. Statement on wait times in obstetrics and
gynaecology. SOGC Policy Statement No. 204, March 2008. J Obstet
Gynaecol Can 2008;30:248–57.
15. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New
Jersey: Lawrence Erlbaum Associates; 1988.
16. Bernstein C, McDonald J, Nyers P, Wright C, Zerehi S. Access not fear:
non-status immigrants and city services preliminary report. 2006. Available
at: https://we.riseup.net/assets/17034/Access%20Not%20Fear%20
Report%20%28Feb%202006%29.pdf. Accessed December 31, 2010.
17. Rousseau C, ter Kuile S, Munoz M, Nadeau L, Ouimet MJ, Kirmayer L,
et al. Health care access for refugees and immigrants with precarious
status: public health and human right challenges. Can J Public Health
2008;99:290–2.
18. Kotelchuck M. The Adequacy of Prenatal Care Utilization Index: its US
distribution and association with low birth weight. Am J Public Health
1994;84:1486–9.
19. Kuiper H, Richwald G, Rotblatt H, Asch S. The communicable disease
impact of eliminating publicly funded prenatal care for undocumented
immigrants. Matern Child Health J 1999;3:39–52.
20. Parchment W, Weiss G, Passannante M. Is the lack of health insurance
the major barrier to early prenatal care at an inner-city hospital? Womens
Health Issues 1996;6:97–105.
21. Hyman I. Immigration and Health. Working Paper 01–05. Health Policy
Working Paper Series. Ottawa: Health Canada; 2001.
22. ACOG Committee Opinion No. 425. Health care for undocumented
immigrants. Obstet Gynecol 2009;113:251–4.