NURS 412 Incivility in Nursing Practice in a Hospital.pdf
Project 9 Poster SRF
1. MANSI CHAUHAN & AMBER PRUITT-RIGGINS
BIOMEDICAL AND HEALTH INFORMATION SCIENCES, UNIVERSITY OF ILLINOIS AT CHICAGO, SPRING 2016
MULTIPLE CHRONIC CONDITIONS: COST, MORTALITY & RACE
As the prevalence of multiple chronic conditions (MCC) rises, its
association with higher healthcare expenditures and lower patient
outcomes becomes a growing concern. This intensifies the need for
more research exploring the impact of MCC on hospital costs and
quality and examining demographic variations. The purpose of this
study was to determine whether there are cost, mortality, and race
variations among hospitalized patients with MCC. The data set of 788
cases was randomly selected from the Healthcare Cost and Utilization
Project (HCUP) National Inpatient Sample (NIS) 2012. IBM SPSS
Version 23 was used to conduct secondary data analysis. Independent
samples t-test results indicated there was a significant difference in
average total charges between inpatients with 1-4 chronic conditions
(CC) and 5+ CC. Chi-square test results showed no association in
death during hospitalization among inpatients with 1-4 CC and 5+ CC
and also no association between Hispanic and Black race among
inpatients with 5+ CC. Despite that these findings showed no
significant results in mortality and race, they do support the trend of
higher healthcare costs among inpatients with MCC. Given the need
to control hospital costs, further exploration of variation in charges
and of factors that may be related to MCC among inpatients is
recommended.
DISCUSSION
The results indicated that average total charges for inpatients
with 5+ CC were significantly higher than those with 1-4 CC, which
complemented previous research. While the Chi-square test results
indicated that deaths were higher for inpatients with 5+ CC than 1-4
CC, there was no significant association. Likewise, while 5+ CC was
more prevalent among Black inpatients than Hispanic inpatients,
there was no significant association. These results were inconsistent
with previous research, which indicated a significant association
between Hispanic and Black race among patients with MCC.
The results in this research may be limited due to a small
dataset, which may not have accurately represented the entire
population. Inconsistencies may also have been caused by comparing
different groups of MCC than previous research. This research
grouped MCC into 1-4 CC and 5+ CC, while other research compared
groups, such as 2-3 CC and 4+ CC.
SAMPLE
• Source: Healthcare Cost and Utilization Project (HCUP) National
Inpatient Sample (NIS) 2012 - 20% sample of discharges from all
inpatient hospitals participating in HCUP (excludes rehabilitation and
long term care)
• Sampling: random sampling stratified by U.S. Census Division
• Data set: randomly selected from NIS 2012
• Project sample limited for assignment - 788 cases with 1+ CC
METHODS
• Quantitative research using secondary data analysis - data processed
using IBM SPSS Version 23
• Descriptive statistics, independent samples t-test, and Chi-square
used to analyze data
• Confidence level = 95%, alpha level = 0.05 for significance testing
S A M P L E / M E T H O D S
Friedman, B., & Steiner, C. (2013) Hospital Utilization, Costs, and Mortality for
Adults With Multiple Chronic Conditions, Nationwide Inpatient Sample,
2009. Preventing Chronic Disease, 10, E62. Retrieved from
http://www.ncbi.nlm.nih.gov.proxy.cc.uic.edu/pmc/articles/PMC3652722
HCUP National Inpatient Sample (NIS). Healthcare Cost and Utilization Project
(HCUP). (2012). Agency for Healthcare Research and Quality, Rockville, MD.
Retrieved from http://www.hcup-us.ahrq.gov/nisoverview.jsp
Jiang H. J., Weiss A.J., Barrett M.L., Sheng M. (2015) Characteristics of Hospital
Stays for Super-Utilizers by Payer, 2012. HCUP Statistical Brief #190. Agency
for Healthcare Research and Quality, Rockville, MD. Retrieved from
http://www.hcup-us.ahrq.gov/reports/statbriefs/sb190-Hospital-Stays-Super-
Utilizers-Payer-2012.pdf
Steiner C., Barrett M., Weiss A., & Andrews R. (2014) Trends and Projections in
Hospital Stays for Adults With Multiple Chronic Conditions (MCC), 2003–
2014. HCUP Statistical Brief #183. Agency for Healthcare Research and
Quality. Retrieved from http://www.hcup-
us.ahrq.gov/reports/statbriefs/sb183-Hospitalizations-Multiple-Chronic-
Conditions-Projections-2014.pdf
Ward B. W., & Schiller J. S. (2013) Prevalence of Multiple Chronic Conditions
Among US Adults: Estimates From the National Health Interview Survey,
2010. Preventing Chronic Disease, 10. 120203. Retrieved from
http://www.cdc.gov/Pcd/issues/2013/12_0203.htm
P U R P O S E / H Y P OT H E S E S
PURPOSE The purpose of this research is to determine whether there are
variations in cost of care and mortality rates among inpatients with multiple
chronic conditions (MCC) discharged from acute care hospitals in the U.S. in
2012. This research will also determine if there are racial disparities among
inpatients with MCC.
RESEARCH QUESTION Are there cost, mortality rate, and race variations
among inpatients with MCC?
HYPOTHESES
• H0: There is no difference in average total charges between inpatients with 1-
4 CC and those with 5 or more CC among discharges from acute care hospitals
in the U.S. in 2012.
• H1: There is a difference in average total charges between inpatients with 1-4
CC and those with 5 or more CC among discharges from acute care hospitals in
the U.S. in 2012.
• H0: There is no association in death during hospitalization between inpatients
with 1-4 CC and those with 5 or more CC among discharges from acute care
hospitals in the U.S. in 2012.
• H2: There is an association in death during hospitalization between inpatients
with 1-4 CC and those with 5 or more CC among discharges from acute care
hospitals in the U.S. in 2012.
• H0: There is no association between Hispanic and Black inpatients with 5 or
more CC discharged from acute care hospitals in the U.S. in 2012.
• H3: There is an association between Hispanic and Black inpatients with 5 or
more CC discharged from acute care hospitals in the U.S. in 2012.
MCC
1-4, 5+ CC
RACE
HISPANIC/BLACK
DEATH
DURING
HOSPITALIZATION
TOTAL
CHARGES
MEAN PER
GROUP
A B S T R A C T
M O D E L
D I S C U S S I O N / C O N C LU S I O NB A C KG R O U N D
R E F E R E N C E S
R E S U LT S
The prevalence of patients with multiple chronic conditions (MCC) has
continuously increased over time and is present in twenty-five percent of
Americans adults (Steiner et al., 2014). MCC refers to the existence of two
or more chronic conditions that affect a patient simultaneously. The
presence of MCC has been seen to impact multiple areas in healthcare,
including quality and cost of care. Demographic variations, including race,
have also been observed among those with MCC. The following trends were
found in previous studies:
• Higher healthcare expenditures among those with MCC than those
without MCC, contributed by:
• Greater percentage of hospital stays
• More expensive hospital stays (Steiner et al., 2014)
• Higher mortality rates among those with MCC than those without MCC
(Friedman & Steiner, 2013)
• Higher prevalence of MCC among non-Hispanic black adults compared to
Hispanic adults (Ward & Schiller, 2013)
These findings are significant as healthcare expenditures among those
with MCC have been increasing over time (Steiner et al., 2014). With the
continuous increase in patients with MCC, hospital mortality rates may
follow the same pattern. Thus, studying these areas may help to find
variations among those with MCC. Also, if racial disparities are found,
further research can be done to determine their causes. Discovering
variations will allow appropriate action to be taken, helping to regulate
healthcare costs and patient outcomes.
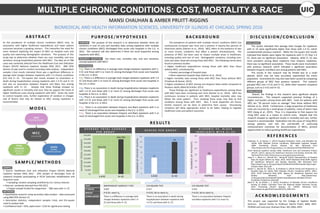
6
12
0
2
4
6
8
10
12
14
1-4 CC 5+ CC
NUMBEROFPATIENTDEATHS
$32,416
$44,794
$0
$5,000
$10,000
$15,000
$20,000
$25,000
$30,000
$35,000
$40,000
$45,000
$50,000
1-4 CC 5+ CC
AVERAGETOTALCHARGES
A V E R A G E T O T A L C H A R G E S
P E R G R O U P
H I S P A N I C V S . B L A C K
I N P A T I E N T S W I T H 5 + C C
D E A T H S P E R G R O U P
TEST INDEPENDENT SAMPLES T-TEST CHI-SQUARE TEST CHI-SQUARE TEST
P-VALUE 0.002 0.317 0.352
RESULT P<0.05, reject H0 P>0.05, fail to reject H0 P>0.05, fail to reject H0
CONCLUSION There is a difference in average total
charges between inpatients with 1-4
CC and those with 5+ CC.
There is no association in death during
hospitalization between inpatients with
1-4 CC and those with 5+ CC.
There is no association between Hispanic
and Black inpatients with 5 or more CC.
29
49
0
10
20
30
40
50
60
HISPANIC BLACK
NUMBEROFPATIENTS
A C K N O W L E D G E M E N T S
This project was supported by the College of Applied Health
Sciences. Special thanks to Professor Valerie Prater, MBA, RHIT,
FAHIMA and instructor Shaheen Khan, MS, MBA, MPH.
CONCLUSION
Overall, the findings in this research were significant despite
inconsistencies. This research supported previous findings of a
higher cost burden among those with MCC. Costs for patients with
MCC are “20 percent more on average” than those without MCC
(Steiner et al., 2014). Furthermore, a large proportion of healthcare
costs are incurred by a small group of patients, many of which have
MCC (Jiang et al., 2015). Thus, it is imperative to find reasons for
rising MCC cases as a means to control costs. Despite that this
research showed no significant results in mortality and race, further
research is recommended. Exploration into the cause of rising MCCs
among patients, and into the cost-benefit of continuing
reimbursement incentives for documentation of MCCs, present
opportunities to reduce growing healthcare expenditures.