Download to read offline








![false + CTPA for PE
5-26%Gimber LH et al. . Perm J [Internet] 2009;13(4):4–10.
Costantino G et alAm J Emerg Med [Internet] 2009;27(9):1109–11.
Ruiz Y et al. Eur Radiol 2003;13(4):823–9.
Ghanima et al. Acta radiol 2007;48(2):165–70.
Hutchinson et al. Am J Roentgenol 2015;205(2):271–7.](https://image.slidesharecdn.com/smaccpenextgen-200128155832/75/Pulmonary-Embolism-Next-Generation-44-2048.jpg)




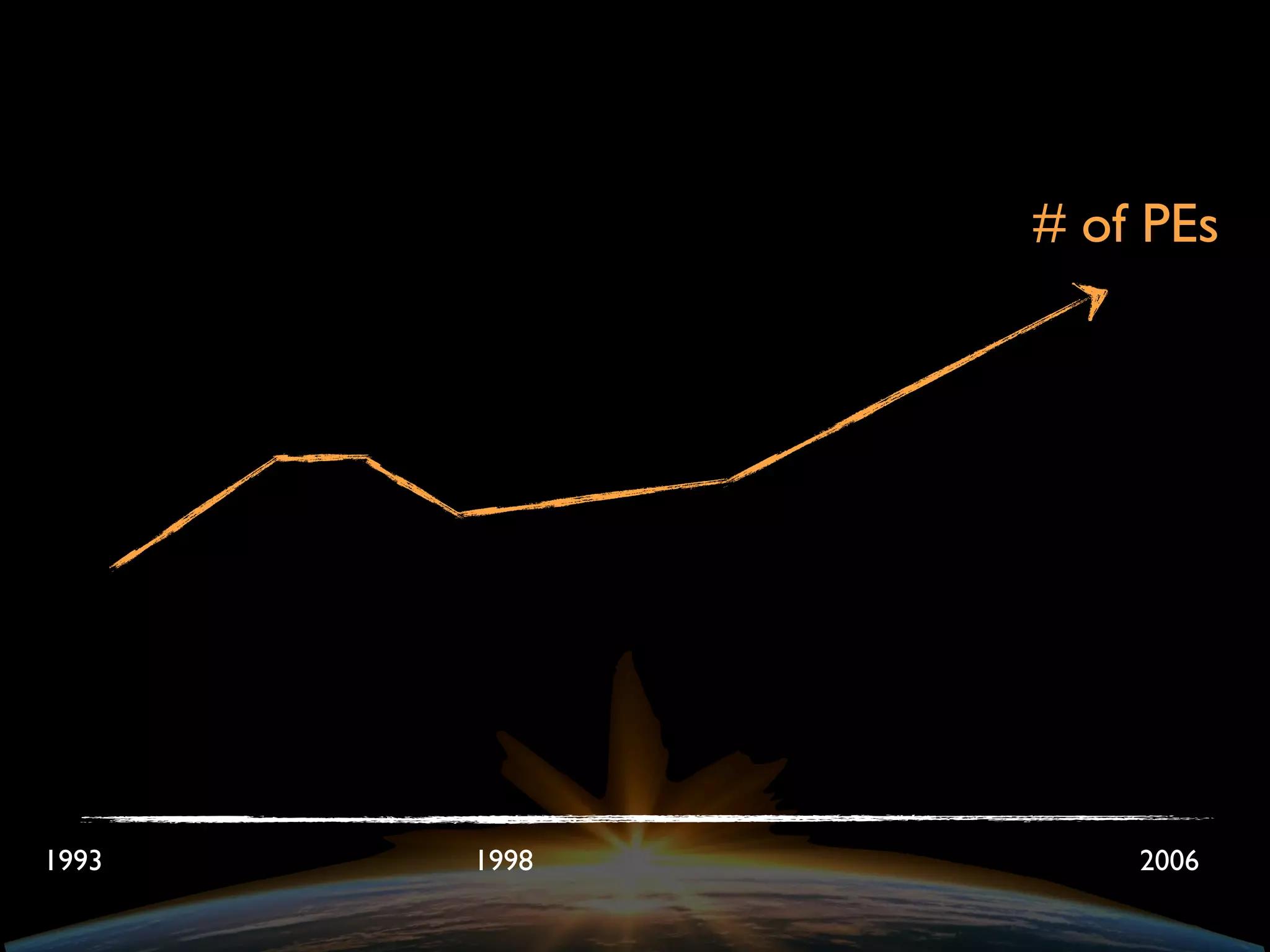
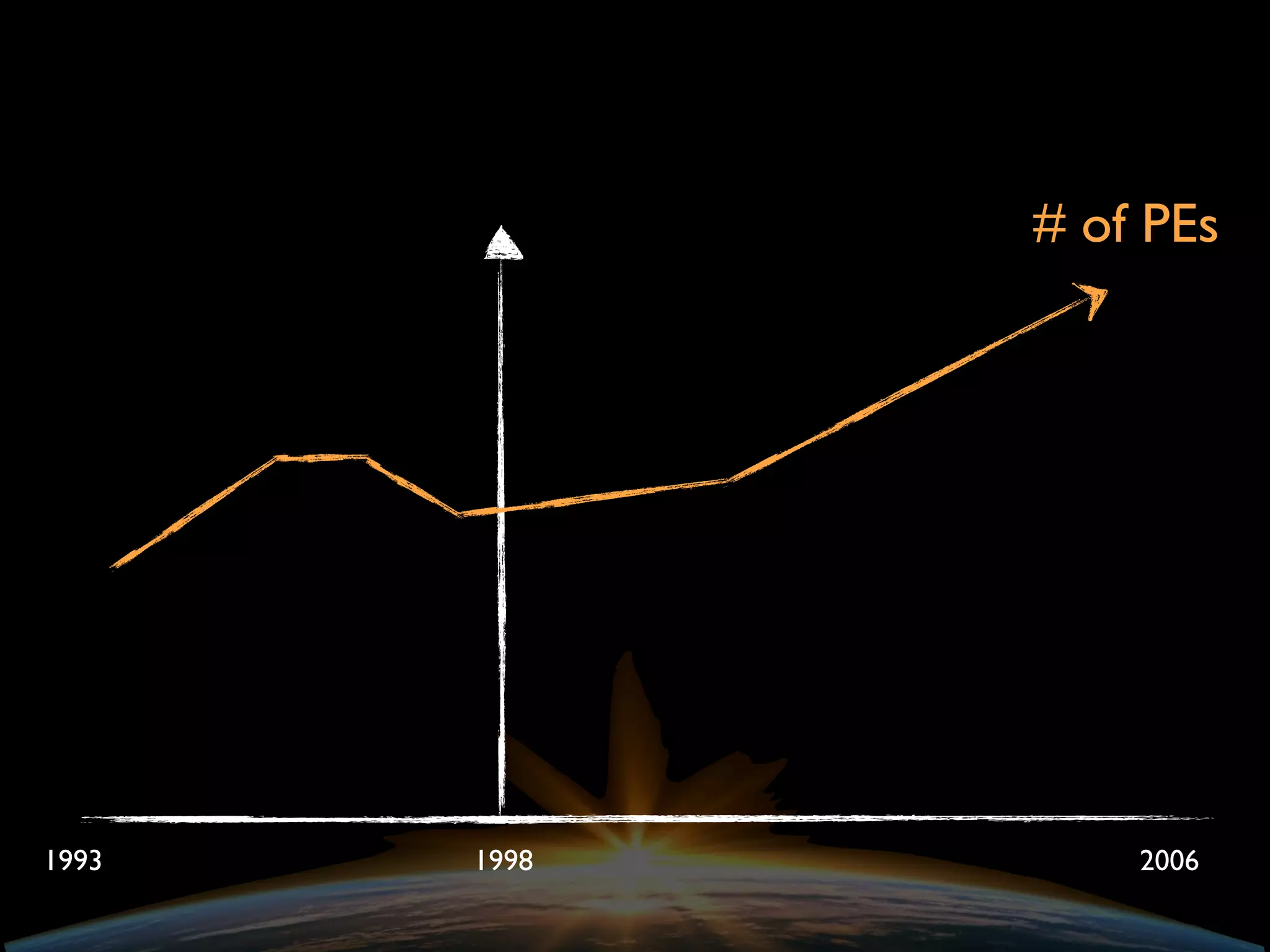
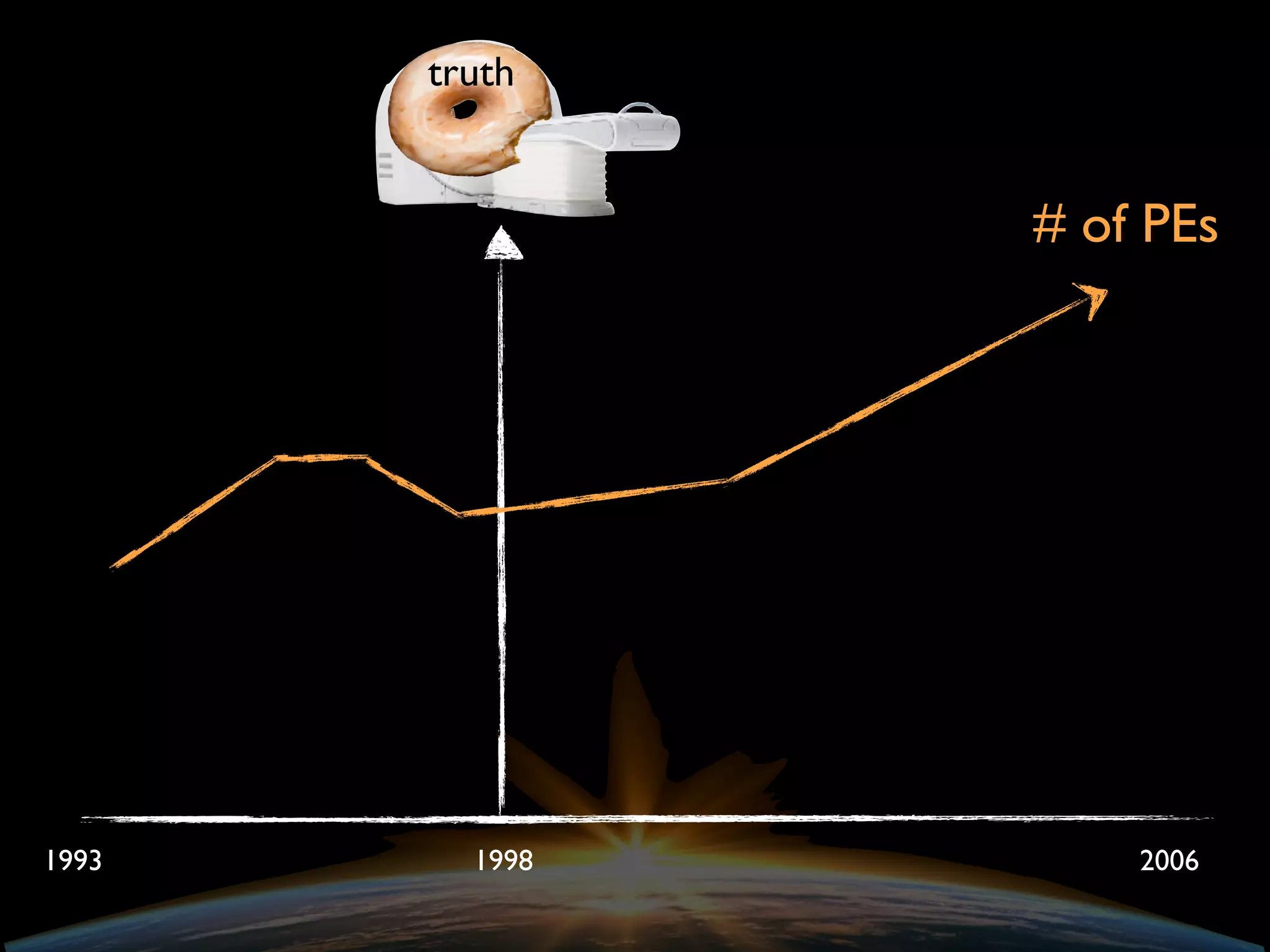
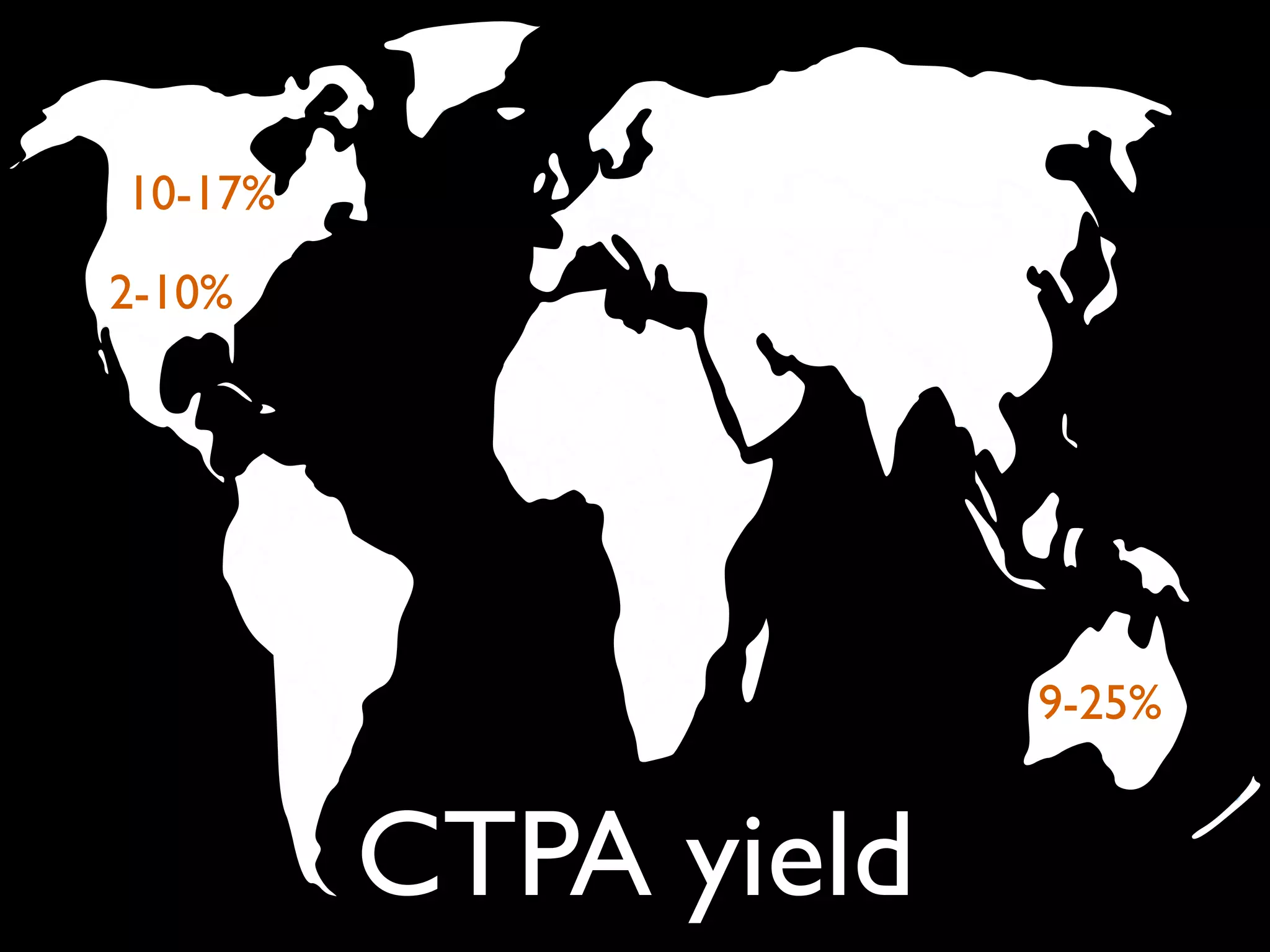
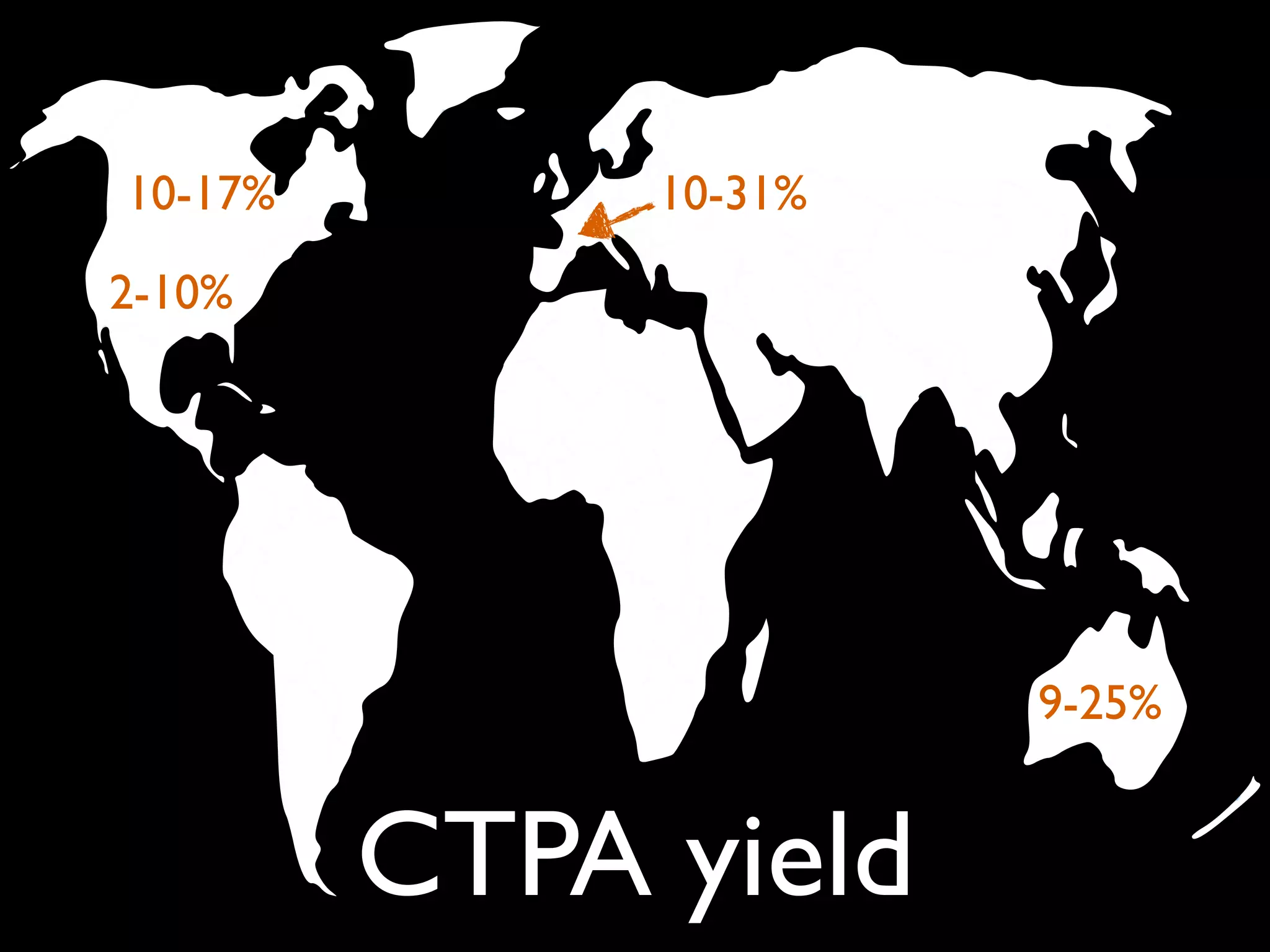
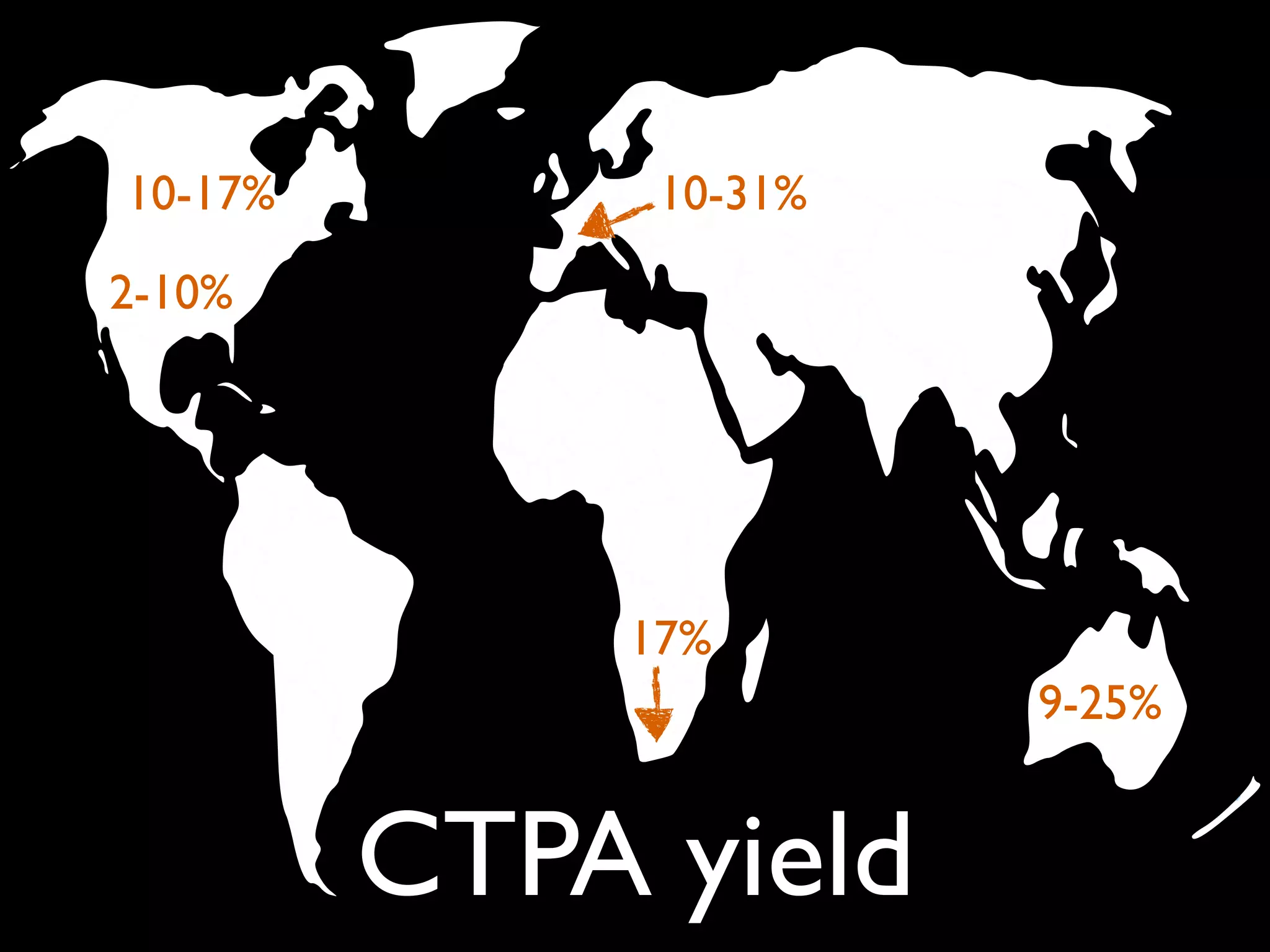
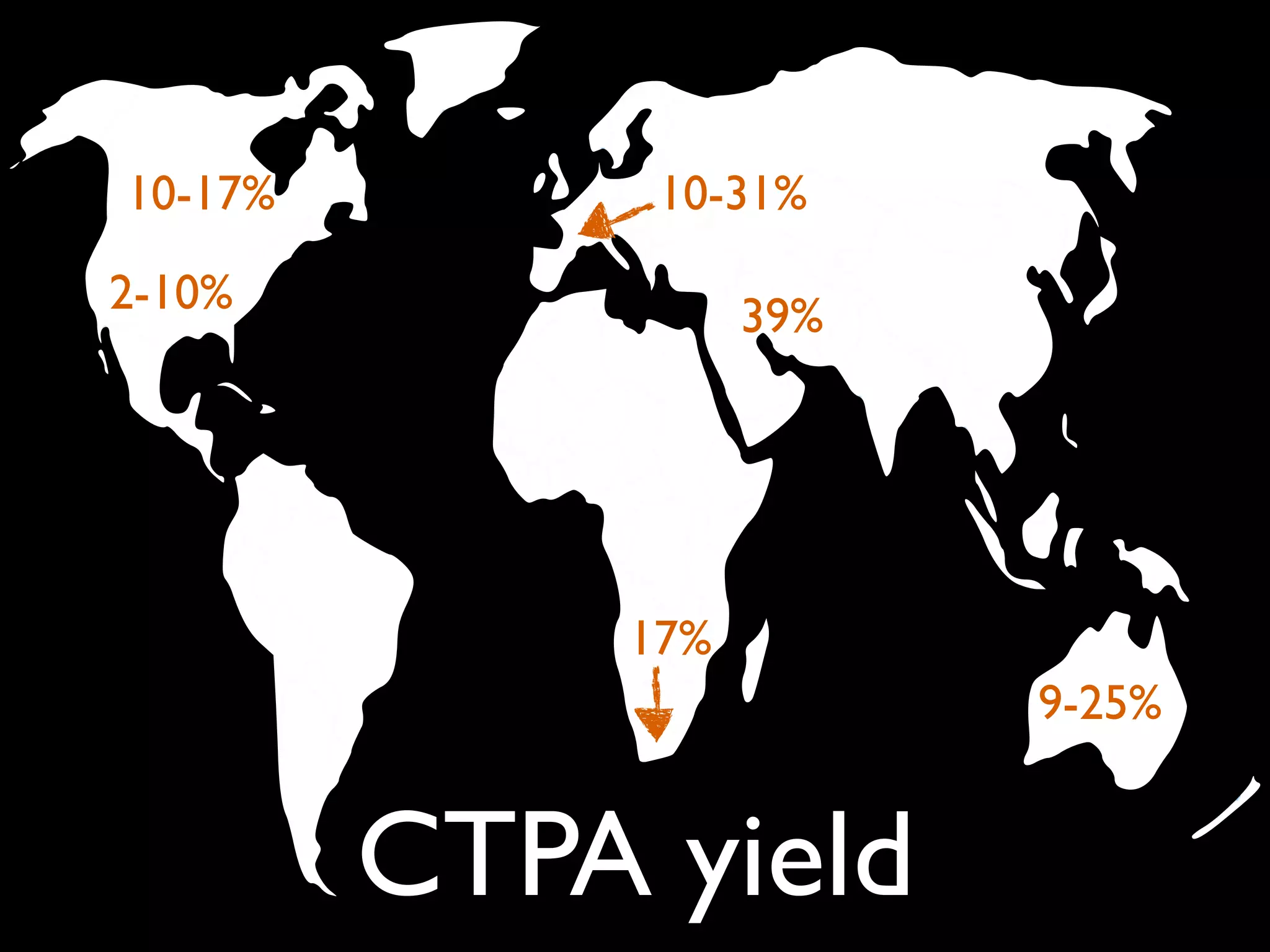
The document discusses the challenges of diagnosing pulmonary embolism (PE), highlighting issues such as overtesting, overdiagnosis, and overtreatment. It references various studies and recommendations regarding risk stratification, the use of D-dimer, and the yield of CT pulmonary angiography (CTPA) in different patient populations. Additionally, it addresses the implications of false positives and unnecessary anticoagulation treatments.












































































![Rheumatic Fever CASE PRESENTATION [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationautosaved-251123182512-9d9b0da4-thumbnail.jpg?width=640&height=640&fit=bounds)










