2. INTRODUCTION
Heterogenous syndrome of unknown etiology.
This multifactorial syndrome emerges at
puberty and has cardiovascular and metabolic
sequelae .
PCOS is a most common endocrine disorder in
women related to fertility.
Leading cause of anovulation, hirsutism and
infertility.
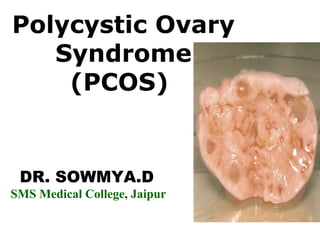
3. Definition of PCOS The original description given by
Stein and Leventhal included obesity, amenorrhoea,
infertility and hirsutism in association with bilateral
enlarged cystic ovaries showing a typical histological
appearance of thickened capsule, multiple cysts and
dense hypertrophied interstitial tissue.
PCOS is the most important among the causes of anovulation
and Speroff quotes that a cross section of ovaries in
anovulatory women at any point will reveal polycystic ovaries
(approximately 75%).
4. The concerns in adolescent with PCOS are twofold-
1. The first involves cyclic control of irregular
menstruation cycles.
2. The second issue involves the avoidance of the long-term
sequelae that are associated with-a)
obesity,
b) insulin resistance,
c) glucose intolerance, and
d) type 2 diabetes.
American Family Physician, 2003, 68(4), 697.
5. Largely unknown
Complex multigenic disorder so far, no
single gene defect has been identified.
Evidence suggest the role of heredity in
PCOS.
6. Intrauterine androgen excess may be the
earliest gestational factor linked with the
pathogenesis of PCOS.
Primary theca cell defects.
Neuroendocrine dysfunction of
hypothalamic - pitutary - ovarian axis ®
Hyperandogenemia.
11. • Congenital origin of syndrome. Some PCOS may
begin in utero.
• Initial presentation as low birth weight.
• In childhood - rapid catch-up of growth ®
Obesity and premature pubarche.
• In Adolescence: -
- Anovulatory symptoms
- Hyperandrogenism
• In adulthood - infertility, cardio-vascular
dysfunction / Type-2 diabetes.
12. Studies of particular interest shown prevention
of this natural progression after early pre-pubertal
treatment with metformin.
Premature pubarche (PP presence of pubic hair
before the age of 8) is considered a forerunner
of PCOS.
As SGA and prematurity were associated with
PP - various authors proposed that PP could be
a marker of hyperinsulinism.
This evolutionary pathway of PCOS from fetal
life to adulthood remains speculative and this
should be further explored.
13. • Variable presenting signs and symptoms.
• PCOS should be consider in adolescent with: -
* Hirsutism
* Precious puberty
* Persistent acne
* Menstrual irregularity
* Acanthosis nigricans
* Obesity
• Some with PCOS may appear clinically normal (no
signs of hyperandrogenism or hyperinsulinism).
14. • The diagnostic approach in should be
based on history and physical exam
• Avoid numerous laboratory tests that do
not contribute to clinical management
Guzick DA. Clinical Updates in Women’s Health Care. ACOG 2009
15. • Focus on several aspects regarding
menstruation such as
– age at menarche,
–length of time between periods,
–quantity of menstrual flow, and
–presence of dysmenorrhea
.
16. Obtaining information regarding-
• Development of secondary sexual
characteristics
• Obesity
• Manifestations of hyperandrogenism
• Family history as it relates to PCOS and
diabetes
• Diet and exercise patterns
• Alcohol consumption and tobacco use
17. A. Menstrual Irregularities
• Persistent irregular cycles two years after menarche.
• Amenorrhoea (Primary or Secondary).
• Oligomenorrhoea (£ 6 cycles / year).
• Dysfunctional uterine bleeding secondary to
endometrial hyperplasia in anovulatory cycles.
B.Resistant - ACNE - may present to primary physician
or dermatologist.
C. Hirsutism - increase in the number of terminal hair
on the face, chest, arms and legs..
D. Precocious puberty or premature adrenarche.
18. Look for clinical manifestation of
hyperandrogenism and signs of
hyperinsulinism.
• Note blood pressure and BMI
• Acne (severe)
• Virilization - Clitoromegaly. Male pattern
baldness.
• Thyroid examination for enlargement or
nodule.
19. Hirsutism
• Presence of terminal
(coarse) hairs in females
in a male-like pattern.
• Prevalence 5 – 15% of
women.
20. • Hirsutism - Ask H/o removal of hair - show pictorial
representation of Ferrimman-Galway Scoring System.
of ³ 8 is consider hirsule.
Hatch et al, 1981 Am J Obstet Gynecol 140: 815-30
21. • Signs of Hyperinsulinism -
Acanthosis nigricans - in
the neck, axilla, chest,
back, perineal area, hand
and feet.
22.
23. Stein and Leventhal (1935)
PCOS in adult women as a syndrome consisting
of amenorrhoea, hirsutism and polycystic
ovaries.
NIH Criteria (1990)
Chronic oligomenorrhoea / anovulation.
Clinical and/or biochemical signs of
hyperandrogenism.
and exclusion of other etiologies : congenital
adrenal hyperplasia, androgen-secreting
tumors, cushing's syndrome.
24. Rotterdam Criteria (2003)
Redefined PCOS as a syndrome with two of
three prerequisites: -
Oligo/anovulation and/or
clinical and/or biochemical signs of
hyperandrogenism.
Polycystic ovaries by ultrasound
and exclusion of other etiologies.
Rotterdam consensus - PCOS is a
functional disorder.
25. In 2006
Androgen excess society provided a
contemporary version of definition of PCOS.
Hyperandrogenism, clinical or biochemical, in
combination with ovarian dysfunction,
including both functional and
ultrasonographic abnormalities, as the core
characteristics of PCOS.
Since there are no established criteria for the
diagnosis of PCOS in adolescents, the adult
criteria are applied to adolescent as well.
26. No consensus regarding specific lab test for PCOS
• To document hyperandrogenism.
• To rule out other endocrinopathies.
• Look for metabolic abnormalities (commonly
seen with PCOS).
• The underlying defects in PCOS are still unclear,
however insulin resistance and metabolic
syndrome are common in both obese and non-obese
PCOS patients, so that evaluation of
glucose tolerance is recommended.
27. A. Total and/or Free Testosterone which may be elevated.
B. Serum sex hormone binding globulin (SHBG) may be
decreased.
C. An increased ratio of LH to FSH of >2 is found in 60% to 70%
of women with PCOS and is more commonly seen in non-obese
women.
D. Lipid panel to rule out dyslipidemias.
E. 2-hour OGTT to rule out diabetes or impaired glucose
tolerance.
F. Prolactin should be checked to rule out prolactinomas.
G. Thyroid function tests, because both hyper and
hypothyroidism are associated with menstrual irregularities.
H. Dehydroepiandrosterone sulfate (DHEA-S) to assess adrenal
androgens
I. Fasting 17 OH-Progesterone to assess 21- Hydroxylase
function in the adrenal gland.
28. Ultrasound
• Ultrasound, especially transvaginal
ultrasound, is a sensitive and specific tool
for detecting polycystic ovaries (PCO).
• Limitations: Transvaginal ultrasound is not
widely used in the adolescent population .
Transabdominal ultrasound is limited by
the inability to visualize at least one ovary
in 16% of women.
29. Ultrasound Criteria for
Diagnosis of PCO
• Twelve or more subcapsular
follicular cysts 2 − 9 mm in diameter
and / or
• Increase in ovarian volume up to
10ml3 (determined by transvaginal
ultrasound).
33. No established therapeutic rules
• Treat - Anovulation
- Hyperandogenemia
- Insulin resistance
Pathophysiologically
Interconnected
34. Maintenance of Normal Weight
First therapeutic priority -
Weight Loss and Lifestyle Modification
10% loss over 6m to 1yr ® improves
menstrual functions, insulin resistance and
metabolic aberrations.
Not only the quantity (calorie excess leading
to obesity), but also the quality of food may
contribute to the pathogenesis of PCOS.
35. • Westernized diet and certain types of
Indian foods contain abundant amount
of Advanced glycated end products
(AGEs) is ovoided.
• AGEs are oxidative molecules, induces
proinflammatory and proatherogenic
cascade.
• High levels of AGEs in lean, non-diabetic
women with PCOS may bear significant
cardiometabolic implications.
36. Second step in therapeutic approach -
Drug administration -
Insulin Sensitizers -
Mainly Metformin - offer holistic therapeutic approach to
PCOS.
Insulin sensitisation
Androgen Decrease
Improvement of menstrual regularity
37. Insulin Sensitizing Agents contd..
• Metformin is an oral biguanide, well established for the
treatment of diabetes.
• Insulin concentrations are therefore decreased with a
resulting
– decrease in androgen
– decrease in LH
– increase in sex hormone‐binding globulin
• It may also have a direct action on theca cells, reducing
androgen production.
• There are now many reports of clinical improvement with
metformin in, mostly obese, adult women with PCOS.
Cochrane Database Syst Rev, 2003, 3,CD003053. Cont….
38. Anti-Androgens and OCPs
Traditional treatment for symptom management.
Flutamide -
• Blocks at the level of the nuclear receptor.
• Nonsteroidal antiandrogen,inhibitor of testosterone
bio synthesis,
Beneficial effects on ovulatory function and metabolic
aberrations (in H/o Premature Pubarche).
• Doses ‐ 250 mg twice/thrice day
• Flutamide + Metformin ® Maximises therapeutic
benefits
39. Cyproterone Acetate (CPA)-
• Synthetic progestin,competative inhibition at
androgen receptor,Most commonly used anti‐androgen
combined with ethnyl estradiol.
• Reverse sequential regimen(CPA 100mg/day 5‐15)and
EE 30 to 50mg/day on cycle of 5 to 26),allows regular
menstrual bleeding, excellent contraception and
treatment of acne and hirsuitism .
Combined Oral Contraceptive
• Suppressing LH Secretion
• Increasing SHBG
• Circulating androgen levels are reduced.
Decreasing free
• testosterone
Estrogen decrease conversion of testosterone to DHT
40. Beneficial Effect on: -
• Hirsutism
• Acne
• Regular shedding of endometrium via withdrawal
bleeds.
OC with newer Progestin
EE + Desogestrel
EE + Cypterone Acetate
EE + Drospirenone
41. MEDROXYPROGESTERONE ACETATE
•It directly affects hypothalopituitary axis by decreasing
GnRH production and release of gonadotropins.
•20 – 40 mg daily in divided doses oraly
•150mg,IM every 6 weeks to 3months in the depot form.
SPIRONOLACTONE
Antagonist of aldosterone,effective in hirsuitism.50-
100mg twice daily.
KETOCONAZOLE
Inhibits steroidogenic cytochromes,200mg/day.reduces
testosterone,androstenedione
42. • DEXAMETHASONE: PCOS who have either
adrenal or mixed adrenal and ovarian
hyperandrogenism,0.25mg nightly.
• FINASTERIDE: Inhibitor of type 2,
5alphareductase enzyme
activity.7.5mgdaily,decreases hirsuitism.
44. 44
Laproscopic Ovarian Drilling
• Treatment option in
– Clomiphene resistant women
– Hyperandrogenic women
• Decreases serum testosterone and increases FSH
level
• 4‐10 punctures in both ovaries.(8mm needle,100 w
cutting current for entry,40w coagulating current
over 2 seconds,(8mm depth,4mm diameter)
• Side effects‐ Post operative adhesions are seen
OVARIAN WEDGE BIOPSY
MECHANICAL METHODS OF HAIR REMOVAL
45. Long Term Consequences of PCOS
PCOS
Chronic Anvoulation Hyperandrogenism IR / HI
NIDDM
Cholestrol
HDL
PAI-I
BP
Hirsuitism
Acne
Alopecia
Cardiovascular
Discase
Unopposed Estrogen
UTERUS BREAST
Oligomenorrhoe
Amenorrhoeaa
Abnormal uterine
bleeding
Interfility
Endomitrial
Hyperplasia
Endometrail
Carcinoma
Breast Carcmoma