2. Why do you need to know about
diabetic feet?
Foot complications are the most common reason
for hospitalisation of diabetic patients
Diabetes is the leading risk factor for major
amputation
Half of all diabetics with a major amputation lose
their other leg within five years
One year survival for diabetic patients with critical
leg ischaemia is around 50%
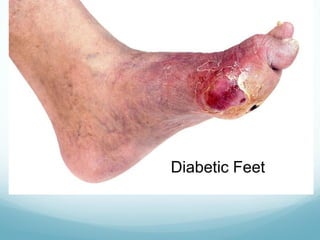
Neuropathy, ischaemia and infection leads to
ulceration, necrosis and gangrene
3. Neuropathy
Neuropathy affects 80% diabetics
presenting with foot lesions
Sensory: deprives patient of pain reflexes
Motor: intrinsic muscles of the foot leading to
clawing of toes
Autonomic: shunting of blood, anhidrosis,
dehydration, fissuring and less elastic skin,
mineral washout from bones
4. Sesamoid bones move forward so weight borne on
metatarsal heads, especially the second metatarsal
Eventually the ankle thrown into equinus and the bones
collapse: Charcot’s foot
Load bearing then leads to pressure ulceration, made
worse by footwear
5.
6. Ischaemia
Combination of proximal occlusive atherosclerosis:
Tibial vessels more severely affected in diabetes
And distal microcirculatory failure:
Failure of endothelium to respond to vasodilators, e.g. NO
Hyperglycaemia, insulin resistance
Changes in basement membrane by products of glycation
Impaired leucocyte migration
Loss of local axon-mediated vasodilation (nuropathy)
7.
8. Infection
Can arise insidiously
Sole of foot, nailbed
Compartments of the foot constrain pus to track
backwards – not seen by patient or felt in presence of
neuropathy
Obtunded immune response and hyperglycaemia: ideal
breeding ground for synergistic infections of aerobic
and anaerobic bacterial infections
Beware gas gangrene
9.
10. Take a history
Symptoms – especially pain
Main cause for acute deterioration?
Ischaemia/neuropathy/infection
Pre-existing arterial disease?
Pre-existing neuropathy?
What is realistic goal of therapy?
11. Examination
Source for infection?
Look for osteomyelitis
Sausage shaped swelling of whole digit
Chronic discharging sinus
Easy subluxation of joints
Visible or palpable bone on probing
Neuropathy – check with cotton wool/nylon brush
Ulcer – does it bleed? i.e. has blood supply
Pulses – classically no foot pulses felt
12. Adjuncts to examination
ABPI – unreliable as incompressible pedal arteries
Doppler signal – monophasic implies significant
proximal artery occlusion
14. Treatment
Analgesia
Hydration
Oxygen
Control of diabetes
High dose antibiotics IV – Pencillin and Metronidazole.
Consider MRSA.
Wound debridement and toilet
Simple dressings: hydrogel, maggots?
VAC dressings for larger wounds
15. Revascularisation
Discuss at MDT
Distal angioplasty or bypass
Is it possible, i.e. extent of disease, presence of suitable
vein, infection (MRSA)
Distal gangrene – local amputation inc. metatarsal head
Web space gangrene – ray amputation
Major amputations can be life saving
Amputation