
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to evaluation of thrombocytopenia
Similar to evaluation of thrombocytopenia (20)
More from Jhysheng Chang
Recently uploaded
Recently uploaded (20)
evaluation of thrombocytopenia
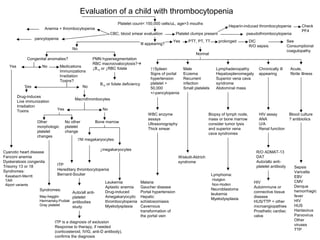
- 1. Evaluation of a child with thrombocytopenia Platelet count< 150,000 cells/uL, age>3 mouths CBC, blood smear evaluation Anemia + thrombocytopenia pancytopenia Platelet clumps present pseudothrombocytopenia Ill appearing? No Congenital anomalies? Yes No PMN hypersegmentation RBC macroovalocytosis? ↓B12 or ↓RBC folate B12 or folate deficiency Medications Immunizations Irradiation Toxins? Yes No Drug-induces Macrothrombocytes Live immunization Irradiation Toxins Yes No Other morphologic platelet changes No other platelet change Bone marrow Cyanotic heart disease Fanconi anemia Dyskeratosis congenita Trisomy 13 or 18 Syndromes: Kasabach-Merritt TAR Alport variants ITP Hereditary thrombocytopenia Bernard-Soulier Syndromes: May-hegglin Hermansky-Pudiak Gray platelet ↑NI megakaryocytes ↓megakaryocytes Leukemia Aplastic anemia Drug-induced Amegakaryocytic thrombocytopenia Myelodysplasia ITP is a diagnosis of exclusion Response to therapy, if needed (corticosteroid, IVIG, anti-D antibody), confirms the diagnosis Yes PTT, PT, TT prolonged DIC R/O sepsis See Consumptional coagulopathy Normal ↑↑Spleen Signs of portal hypertension platelet > 50,000 +/-pancytopenia Male Eczema Recurrent infection Small platelets Lymphadenopathy Hepatosplenomegaly Superior vena cava syndrome Abdominal mass Chronically ill appearing Acute, fibrile illness WBC enzyme assays Ultrasonography Thick smear Biopsy of lymph node, mass or bone marrow consider tumor lysis and superior vena cava syndromes HIV assay ANA U/A Renal function Blood culture ? antibiotics Malaria Gaucher disease Portal hypertension Hepatic schistosomiasis Cavernous transformation of the portal vein Wiskott-Aldrich syndrome Lymphoma: Hodgkin Non-Hodkin Neuroblastoma leukemia Myelodysplasia R/O ADMAT-13 DAT Auto/allo anti-platelet antibody Sepsis HIV Autoimmune or connective tissue disease HUS/TTP + other microangiopathies Prosthetic cardiac valve Varicella EBV CMV Denque hemorrhagic fever HIV HUS Hantavirus Parvovirus Other viruses TTP Auto/all anti-platelet antibodies study Heparin-induced thrombocytopenia Check PF4
- 2. Thrombocytopenia in the well neonate Platelet count < 150,000/uL History, examination, CBC, blood smear evaluation, maternal platelet count If there is on obvious etilogy for the TP, bacterial sepsis Congenital anomalies must be considered Maternal history positive Maternal TP Neonatal TP in siblings Maternal drug use Mild TP no bleeding Observe if no change Maternal ITP or SLE Mother acutely ill MASPAT or Capture-P for auto anti-platelet antibodies Preeclampsia HELLP syndrome DIC Hyperthuroidism Viral Illness Platelet <50,000: IVIG ?corticosteroids Random donor platelet transfusions if bleeding( which is unusual ) Blueberry muffin lesions congenital infection hemangiomas Kasabach-Merritt syndrome Purpura fulminans Multiple malformations Trisomy 21,13,18 45XO 11q23.3 deletion TAR syndrome Placenta abnormal Neonatal autoimmune TP Drug adsorption MASPAT or Capture-P Drug-induced TP Placenta infarcts Chorangioma Platelets < 50,000 IVIG < 20,000 Transfuse maternal platelet Platelet Ag and Ab studies on parents and/or baby ( MASPAT or Capture-P cross matching) NAIT Maternal history negative Blood culture, prophylactic antibiotics Abnormal CBC/smear Abnormal Hb, WBC, ANC, RBC indiced or RBC fragments Abnormal platelet size +/- other morphologic changes Bone marrow infiltration Aplastic anemia Pearson syndrome Congenital micro-angiopathic anemia Syndromes Large platelets Bernard-Soulier May-Hegglin Hermansky-Pudiak Gray platelet Small platelet Wiskott-Aldrich NI CBC and smear Platelet > 20,000~30,000 no bleeding Platelet <20,000~30,000 +/- clinical bleeding Careful observation clinically and follow platelet count Count stable or increasing Transfuse random donor platelets Persistent platelets↑ No or transient platelets ↑ Transfuse washed, irradiated maternal platelets IVIG 1g/kg X 1~3 days Persistent platelets post-transfusion ↑ No or only transient platelets↑ Neonatal autoimmune TP Kasabach-Merritt syndrome Early sepsis Viral infection Unknown etilolgy Toxoplasmosis NAIT Drug-induced Amegakaryocytosis Macrothrombocytopenia Familial TP
- 3. Thrombocytopenia in the ill neonate Any etiology of thrombocytopenia that occurs in the well child History, examination, CBC, blood smear evaluation See Thrombocytopenia in the well neonate Platelets 100,000~149,000/uL Platelets < 100,000/uL If platelets < 50,000? Cranial ultrasound to R/O intracranial hemorrhage resulting from severe TP of any etology Follow platelet count >150,000/uL no further evaluation 100,000~149,000 continue to fellow PTT, PT, TT High Hb Severe jaundice and low Hb Prolonged PTT, PT and/or TT +/- microangiopathic hemolytic anemia: Consider D-dimer of FSP, and/or fibrinogen +/- factors II, V and VIII Polycythemia Cyanotic congenital heart disease Erythroblastosis fetalis Exchange transfusion p phototherapy DIC Etologies Acute infection Asphyxia RDS Meconium aspiration Obstetrical complications Shock Thrombosis Severe hemolytic disease of the newborn Severe hepatic disease TP usually mild enough not to require transfusion except in DIC due to erythroblastosis fetalis Treat underlying disease Maintain platelets > 50,000 with transfusions Maintain fibrinogen > 1.0g/L and PT WNL with FFP +/- cyrorecipitate Normal PTT, PT, TT RDS Pulmonary hypertansion Meconium aspiration Mechanical ventilation Perinatal asphyxia Infection Viral Bacterial Fungal No other specific etiology identified Unknown etiology Ongoing re-evaluation if platelets < 50,000 Acutely ill Usually premature Abdominal signs NEC Acidosis Emesis Lethargy +/- Central venous catheter Hematuria Pulseless extremity Drug use Gancyclovir Heparin Vancomycin Metabolic defects Thrombosis Drug-induced Stop drug Remove catheter when possible LMWH ??Thrombolytic therapy Supportive care- Platelet transfusions to maintain count > 20,000 in stable full term neonates, > 50,000 with hemorrhage, surgery, or more extremely preterm infants Observe for DIC