Case Review #49: 48 year old female with progressive Adult Idiopathic Scoliosis
•
3 likes•792 views

48 year old female presented to Dr. Pashman with a long history of low back pain. The patient had been treated with a microdiscectomy, epidurals, physical therapy, and medication. The patient was treated with a spinal fusion.

Recommended
Recommended
More Related Content
More from Robert Pashman
More from Robert Pashman (20)
Recently uploaded
Recently uploaded (20)
Case Review #49: 48 year old female with progressive Adult Idiopathic Scoliosis
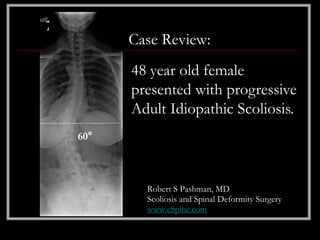
- 1. Case Review: 48 year old female presented with progressive Adult Idiopathic Scoliosis. 60° Robert S Pashman, MD Scoliosis and Spinal Deformity Surgery www.eSpine.com
- 2. Patient History • 48-year-old female • Progressive Adult Idiopathic Scoliosis • The patient has a long history of low back pain and is status post microdiskectomy at L4-5 in 2003 after motor vehicle accident. • The patient has exhausted physical therapy, epidurals, and has taken anti-inflammatory medications. • The patient is very active and fit.
- 3. Pre-op X-rays The x-rays show that the patient has a 60° left lumbar curve with marked rotation. She has severe degeneration of the lumbosacral joint, L4-L5 is significantly tilted and out of plane. The patient has a compensatory upper thoracic curve. The patient has severe 60° thoracolumbar kyphosis measured at greater than 40°; this should be 0°. This has caused significant forward decompensation and hyperlordosis of the lumbar spine which has led to advanced degeneration.
- 4. Indications for Surgery 1. Kim/SRP type 3 progressive adult idiopathic scoliosis with large lumbar rotated curve. 2. Sixth lumbosacral obliquity with severe degeneration. 3. Isthmic spondylolisthesis at L5-S1 with either bilateral or unilateral pars and articularis fractures. 4. Gross instability of lumbar spine due to the above factors plus status post micro decompression L4-5. 5. Now with unremitting low back and leg pain due to greater than 50 degree rotated lumbar curve and fixed thoracic component including thoracolumbar kyphosis.
- 5. Surgical Strategy – Stage 1 • Abdominal retroperitoneal approach to the lumbosacral spine. • Radical diskectomy L5-S1 with subtotal vertebrectomy of L5 to allow entrance into L5-S1 space for reduction and fusion of interbody L4-S1. • Interbody fusion after removal of disk herniation under loop and high intensity light illumination for placement of a PEEK 8 mm device with autogenous and putty bone centrally, and fully threaded screw over a washer. • Radical diskectomy L4-5 with correction of coronal plane decompensation L4-5. • Placement of PEEK device with autogenous bone and allograft at L4-5. • Anterior screw fixation L4-5 and L5-S1. • Intraoperative use of fluoro.
- 6. Indications for Surgery 1. KIM/SRP type 3 thoracolumbar progressive adult idiopathic scoliosis, 65 degrees. 2. Thoracolumbar kyphosis. 3. Status post anterior interbody fusion, L5-S1, L4-5 for horizontalization of index lumbosacral curve. 4. Progressive radiculopathy and pain due to collapsing scoliosis, coronal and sagittal decompensation. 5. Status post hemilaminectomy, L4-5. 6. Failed conservative therapy.
- 7. Surgical Strategy - Stage 2 • T10-pelvis instrumentation using ¼ inch stainless steel pedicle screw/rod construct. • Posterior spinal fusion, T2 - sacral pelvis using locally- harvested autogenous bone and allograft bone in a bone mill. • Interlaminar decompression, reexploration decompression under high- loupe magnification, L4-5, L5-S1. • Multiple-level spinal osteotomy, Smith-Peterson osteotomy, for recontouring, thoracolumbar kyphosis, T12-L1, L1-L2, L2-L3, L4-L5 with bilateral facetectomy and mobilization. • Intraoperative O-arm neuronavigation. • Intraoperative somatosensory evoked potential motor evoked potential use. • Plastic closure of wound.
- 8. Post-op Films • The patient's plumb line improved post-operatively. • Her sagittal plane is perfect. • All the instrumentation looks great.