
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Ct angio ppt
Similar to Ct angio ppt (20)
Recently uploaded
Recently uploaded (20)
Ct angio ppt
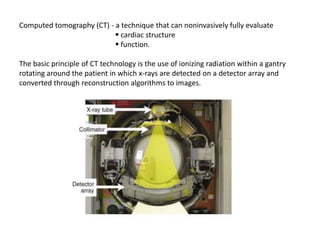
- 1. Computed tomography (CT) - a technique that can noninvasively fully evaluate cardiac structure function. The basic principle of CT technology is the use of ionizing radiation within a gantry rotating around the patient in which x-rays are detected on a detector array and converted through reconstruction algorithms to images.
- 2. Types of CT 1. EBCT (Electron beam CT) 2. MDCT ( Multidetector CT) The most notable technical advance is progressive increase in the number of detector rows (or slices). Each row is a narrow channel, approximately 0.625 mm in width, through which x-rays are detected on scintillation crystals. The number of detector rows aligned in an array has increased from a single detector to 4, 16, and 64 (present standard technology) and now on to “wide” detectors of 256 to 320 rows.
- 3. The increase in the number of rows leads to wider coverage (more of the heart viewed simultaneously, e.g., 64 rows of 0.625-mm width produces approximately 4 cm of coverage, leading to shorter scan acquisition times and consequently reduced radiation exposure and contrast requirements.
- 4. EBCT : EBCT uses an electron beam (current 630 mA, voltage 130 kV) that is deflected via a magnetic coil and focused to strike a series of four tungsten targets located beneath the patient. The electron beam is magnetically swept along the tungsten targets at a 210-degree arc. EBCT has no moving parts.
- 5. MDCT : Multidetector CT (MDCT) scanners produce images by rotating an x-ray tube around a circular gantry through which the patient advances on a moving table.
- 6. Scan Modes There are two basic scan modes in cardiac CT, helical (spiral) and axial (sequential, step & shoot) scanning. Helical (spiral) scanning : Most current MDCT scanners use spiral, retrospectively gated acquisition techniques. Helical scanning involves continuous radiation exposure and table movement (the patient is moved through the rotating x-ray beam), during which the detector arrays receive projection data from multiple contiguous slices of the patient. Axial (sequential, step & shoot) scanning : axial imaging involves sequential scanner “snapshots,” in between which the x-ray tube is turned off and the table is moved to a different position for the next image to be acquired.
- 8. ECG gating a. Prospective triggering: The trigger signal is derived from the patient’s ECG based on a prospective estimation of the RR interval. The scan is usually triggered to begin at a defined point after the R wave, usually allowing image acquisition to occur during diastole. Advantage: ● dose efficient (80% reduction in x-ray exposure) Disadvantage : ● limited portion of cardiac cycle data set obtained ● greatly depends on the regularity of patient’s heart rate
- 9. b. Retrospective gating : Collects data during the entire cardiac cycle. Once scan is complete , data from specific periods of the cardiac cycle are used for image reconstruction by retrospective referencing to the ECG signal. Advantage : allows assessment of cardiac function via four-dimensional reconstruction. Disadvantage : higher radiation dose exposure.
- 10. Contrast enhanced imaging : Administration of iodinated contrast media increases the attenuation of the blood pool, improving vessel delineation and tissue characterization. When using contrast, image acquisition must be timed such that images are acquired when the blood pool enhancement in the target structure is maximal. Various techniques exist to time the arrival of the contrast bolus in the arterial tree and initiate imaging.
- 11. Indications: A. Evaluation of chest pain in patients at low to intermediate pretest probability of disease and persistent chest pain after an equivocal stress test. B. Suspicion of coronary artery anomalies. MDCT has very high sensitivity and specificity for coronary anomalies. C. Pulmonary vein evaluation can be performed, often before or after pulmonary vein isolation for atrial fibrillation. D. Evaluation of cardiac masses when other modalities such as TTE, TEE, or MRI are unrevealing. E. Evaluation of pericardial disease when other modalities such as TTE, TEE, or MRI are unrevealing. F. Assessment of anatomy in complex congenital heart disease.
- 12. G. Presurgical evaluation, particularly before redo open heart surgery. MDCT can aid in describing prior bypass graft location, identifying safe sites for surgical approach. H. Assessing graft patency after prior bypass surgery is feasible in many cases, though sometimes limited by artifacts related to calcium and surgical clips. I. Evaluation of aortic disease. MDCT is the test of choice for evaluating aortic aneurysm and suspected aortic dissection. J. Evaluation of suspected pulmonary embolism
- 13. CONTRAINDICATIONS: Unlike with cardiac MRI, few absolute contra indications exist for cardiac CT. However, there are important risks associated with radiation and/or contrast exposure that must be weighed against the benefits of the scan. Absolute contraindications : A. Renal insufficiency. Given the potential for contrast nephropathy, patients with significant renal insufficiency (i.e., Cr > 1.6 mg/dL) should not undergo contrast-enhanced CT unless the information from the scan is critical and the risks/benefits are thoroughly discussed with the patient. B. Known history of anaphylactic contrast reactions A prior anaphylactic response to contrast is generally felt to be an absolute contraindication to intravenous iodinated contrast administration at many institutions. C. Pregnancy D. Clinical instability
- 14. Relative contraindications A. Contrast (iodine) allergy. Patients with allergic reactions to contrast should be pretreated with diphenhydramine and steroids before contrast administration. B. Recent intravenous iodinated contrast administration. Patients who have received an intravenous dose of iodinated contrast should avoid contrast-enhanced CT scanning for 24 hours to reduce the risk of contrast nephropathy. C. Hyperthyroidism. Iodinated contrast is contraindicated in the setting of uncontrolled hyperthyroidism due to possible precipitation of thyrotoxicosis. D. Atrial fibrillation or any irregular heart rhythm, is a contraindication to coronary CT angiography due to image degradation from suboptimal ECG gating. E. Inability to breath hold for at least 10 seconds. Image quality will be significantly reduced due to respiratory motion artifact if the patient cannot comply with breath hold instructions. F. Morbid obesity G. Severe coronary calcium
- 15. SAFETY A. Radiation exposure : Radiation doses of cardiac CT scans vary greatly depending on the scan parameter settings, scan range (cranial-caudal length of the scan), gender (women receive more radiation due to breast tissue), and patient body habitus (obesity increases exposure). ● chest x-ray is 0.04 to 0.10 mSv, ● average annual background radiation 3 to 3.6 mSv. ● Invasive diagnostic coronary angiography 2.1 to 4 mSv. ● coronary CT angiography 4 to 11 mSv. With use of prospective-ECG triggering, axial imaging modes, and software adaptations, recent studies have reported the feasibility of CT coronary angiography with comparable image quality and substantially reduced radiation doses (i.e., 1.1 to 3.0 mSv). This remains an area of active investigation.
- 16. B. Contrast nephropathy : Iodinated contrast media can cause renal ischemia by reducing renal blood flow or increasing oxygen demand and may also have a direct toxic effect on tubular epithelial cells. If a contrast-enhanced CT study is necessary in patients with significant renal insufficiency, prophylactic measures should be taken ● saline hydration ● n-acetylcysteine ● use of low osmolar agents ● sodium bicarbonate infusion
- 18. CLINICAL APPLICATIONS A. Coronary calcium scoring Coronary calcium is a surrogate marker for coronary atherosclerotic plaque. Coronary artery calcium score is directly proportional to the overall extent of atherosclerosis, although typically only a minority (approximately 20%) of plaque is calcified. Complete absence of coronary artery calcium makes the presence of significant coronary luminal obstruction highly unlikely and indicates a very low risk of future coronary events. Men, CKD, diabetics tend to have higher coronary calcium scores. Contrast is not necessary because calcium is readily identified secondary to its very high x-ray attenuation coefficient (high Hounsfield unit score).
- 20. The Agatston coronary artery calcium (CAC) score is the most frequently used scoring system. It is derived by measuring the area of each calcified coronary lesion and multiplying it by a coefficient of 1 to 4, depending on the maximum CT attenuation within that lesion. Volume score Mass score A coronary calcium coverage score : multivessel coronary calcium, the number of calcified lesions and diffuse spotty pattern (small foci <3 mm) are associated with a higher clinical risk. The CAC score can be classified into five groups: 1) zero, no coronary calcification; 2) 100, mild coronary calcification; 3) > 100 to 399, moderate calcification; 4) >400 to 999, severe calcification; 5) > 1000, extensive calcification.
- 21. In comparison with a CAC score of zero, the presence of any CAC is associated with a fourfold risk of coronary events over 3 to 5 years. In patients at intermediate clinical risk for coronary events (e.g., by Framingham score), the CAC score can help to reclassify patients to a higher or lower risk group. For instance, a CAC score of zero confirms low risk of events. Conversely, a CAC score of greater than 400 is observed with a significant cardiac event rate (greater than 2 %/year) in patients who appear to be intermediate risk by Framingham score. Because statins have no documented effect on CAC progression, there is no value in repeating CAC in persons with a score of greater than 100 or the 75th percentile. However, not every atherosclerotic plaque is calcified, and even the detection of a large amount of calcium does not imply the presence of significant stenoses. Therefore, it adds only incrementally to traditional risk assessment and should not be used in isolation. The test is most useful in intermediate risk populations, in which a high or low score may reclassify individuals to a higher or lower risk group. Unselected screening is not recommended.
- 22. CAC and Stenosis Severity : Significant coronary artery stenosis (>50%) by angiography is frequently associated with the presence of coronary artery calcium. However, the severity of angiographic coronary artery stenosis is not directly related to the total CAC. CAC and Myocardial Ischemia : Good correlation between CT and myocardial perfusion SPECT for identifying both subclinical CAD and silent myocardial ischemia in a generally asymptomatic population who had risk factors for CAD development. Few patients with CACS <400 had a perfusion defect, whereas nearly half of the patients with CACS >400 had an abnormal SPECT.
- 23. Coronary CT angiography : The primary clinical application of cardiac CT is the performance of noninvasive coronary CT angiography among patients with symptoms suggestive of myocardial ischemia. The overall accuracy of 64-row CT angiography included a sensitivity of 87% to 99% and specificity of 93% to 96%. Coronary CT angiography for evaluating CAD is most useful in low- to intermediate-risk patients with angina or anginal equivalent. The negative predictive value of coronary CT angiography is uniformly high in studies, approaching 93% to 100%; in other words, coronary CT angiography is an excellent modality for ruling out coronary disease.
- 25. Patients who are generally poor candidates for coronary CT angiography include 1. those likely to have heavily calcified coronary arteries (older than 75, endstage renal disease, Paget's disease), atrial fibrillation /flutter, frequent ventricular ectopic beats, or uncontrolled tachycardia. 2. Known severe CAD is generally a contraindication to coronary CT angiography. However, cardiac CT has been shown to have high sensitivity and specificity for assessment of bypass graft patency in patients with previous coronary artery bypass grafting (CABG) 3. Patients with prior coronary artery stents are generally poor candidates for CAD, although selected patients with proximal LAD or left main stents may be successfully imaged. Current CT technology does not allow for the accurate quantification of in-stent stenosis severity.
- 26. Noncalcified plaque appears as a low to intermediate attenuation irregularity in the vessel wall. Calcified plaques are bright, high-attenuation lesions in the vessel wall and may be associated with positive remodeling of the vessel. Densely calcified plaques are often associated with calcium blooming artifact, which can lead to overestimation of luminal stenosis severity. The accuracy of coronary CT angiography is highest in the larger proximal to medium vessels, which are more likely to benefit from an invasive management strategy. Coronary stenoses are generally categorized as mild (less than 50% diameter stenosis), moderate (50% t070% stenosis), or severe (greater than 70% stenosis). Similar to results with invasive coronary angiography, the determination of an anatomic stenosis is only modestly predictive of inducible ischemia. A 50% or greater stenosis on cardiac CT has a 30% to 50% likelihood of demonstrable ischemia on myocardial perfusion imaging .
- 27. Detection of Noncalcified Plaque Defined as any coronary arterial wall lesion with an x-ray attenuation detectably below the iodine contrast medium but higher than surrounding tissue. Such plaque is difficult to quantify, with limited accuracy and reproducibility. Detection requires maximal spatial and temporal resolution and minimized image noise with higher radiation exposures. Compared with intravascular ultrasound, the sensitivity of coronary MDCT is approximately 80%. Detection of vulnerable plaques Plaque features proposed to be associated with greater risk for plaque rupture or acute coronary syndromes include ●low-attenuation plaque (plaque <30 HU), ●outward arterial remodeling (artery diameter ratio of the involved segment to a proximal reference of 1.1 or greater), and ●a spotty pattern (<3 mm in size) of calcification. In particular, both low-attenuation plaque and outward arterial remodeling have been associated with increased risk of acute coronary events. A threefold worse cardiovascular prognosis has been found in the setting of a greater number of coronary vessels and of coronary artery segments involved with plaque.
- 28. Bypass graft imaging : 1. Graft location : MDCT can accurately characterize the origin, course, and touchdown of prior bypass grafts 2. Graft patency : Using a protocol similar to that used for coronary artery assessment (less than 1 mm slice thickness), patency of both arterial and venous bypass grafts can be assessed. Recent studies have suggested that the sensitivity and specificity of MDCT for detecting stenosis or occlusion of bypass grafts, when compared with invasive angiography, is 97% and 97%, respectively. Occasionally, artifacts related to metallic clips can interfere with assessment of the distal anastomosis of an arterial graft (internal mammary or radial artery graft).
- 30. Stent patency: Image artifact from metallic stents limits the application in patients with prior coronary stent procedures. Small stents are difficult to evaluate and prone to noninterpretability. However, 90% accuracy can be obtained in stents 3 mm or greater in diameter with the use of sharp kernel and wide display window. Quantitative assessment of within-stent contrast density may assist in the diagnosis.
- 31. Coronary artery anomalies : MDCT is an excellent modality for assessing patients with known or suspected coronary artery anomalies. MDCT can accurately assess the origin and course of anomalous coronaries, and can describe the relationship of the coronary artery to neighboring structures. Although MRI can also be used to assess anomalous coronaries without the need for radiation exposure, the spatial resolution, ease of data acquisition, and reliable image quality of MDCT make it a reasonable first choice. Intramyocardial bridging can also be detected with high sensitivity.
- 32. Cardiac morphology/function : Contrast-enhanced MDCT can provide high resolution morphologic images of the cardiac chambers as well as accurate assessment of right and left ventricular systolic function. However, other imaging modalities such as echocardiography or MRI, which do not require radiation exposure, are generally preferred initially for assessing cardiac morphology. 1. Patients with prior myocardial infarction can have fibrous replacement of myocardium with or without calcification, ventricular wall thinning, aneurysm formation and cavitary thrombus. 2. Ventricular dysplasia is characterized by: fibrous and/or fatty replacement of myocardium, ventricular wall thinning and/or focal aneurysm formation, and ventricular cavity dilation with regional or global wall motion abnormalities. 3. Mass : CT provides somewhat less information about tissue type than cardiac MRI.
- 34. Pericardial diseases : The pericardium appears as a thin line (1 to 2 mm) surrounding the heart, usually visible with a small amount of adjacent pericardiaI fat. The pericardium normally enhances with contrast administration; hyperenhancement of the pericardium in the appropriate clinical setting is characteristic of pericarditis. 1. By CT, congenital absence of the pericardium is easily diagnosed. 2. Findings of pericardial constriction on CT include irregular pericardiaI thickening and calcification, conical or tubular compression of one or both ventricles, enlargement of one or both atria, dilation of the IVC, and a characteristic diastolic bounce of the interventricular septum. 3. Pericardial effusions can be reliably detected by CT. Pericardial tamponade is better evaluated by echocardiography, however, due to its ability to provide hemodynamic information. 4. A pericardiaI cyst will appear as a well circumscribed paracardiac mass with characteristic water attenuation (H.U. = 0), usually in the right costophrenic angle. 5. Both primary neoplasms and, more commonly, metastatic neoplasms can be visualized in the pericardium.
- 36. Congenital heart disease : MDCT may be used in selected patients in whom echocardiography is non-diagnostic or inadequate and MRI is not available. The ability to evaluate cardiovascular anatomy in multiple planes is often helpful for delineating cardiac morphology in congenital heart disease, particularly with regard to the relationship of the great vessels, pulmonary veins, and coronary arteries. Specific situations in which MDCT is helpful include 1. "hard-to-find" adult shunt detection (sinus venosus atrial septal defect, patent ductus arteriosus); 2. visualization of pulmonary arteries in cyanotic congenital heart disease; 3. precise definition of aortic anatomy in Marfan's syndrome or coarctation; 4. definition of partial or total anomalous pulmonary venous drainage.
- 37. Diseases of the aorta constitute a common and important indication for CT examinations. Contrast-enhanced MDCT is nearly 100% sensitive and specific for evaluating acute aortic syndromes. 1. Acute aortic dissection is characterized on CT by visualization of a dissection flap (i.e., separation of the intima from the media) that forms true and false lumens. The CT study can characterize the origin and extent of the dissection, classify it as Type A or B, assess for concomitant aneurysmal aortic dilatation, and identify branch vessels involvement. 2. Aortic intramural hematomas are believed to be caused by spontaneous hemorrhage of the vaso vasorum into the medial layer. They appear as crescent- shaped areas of increased attenuation with eccentric aortic wall thickening. Unlike dissections, hematomas do not spiral around the aorta. 3. Aortic aneurysm is a permanent dilation of 150% of the normal aortic caliber (usually greater than 5 cm in the thoracic aorta and greater than 3 cm in the abdominal aorta). 4. Penetrating atherosclerotic ulcer. These tend to be focal lesions of the descending thoracic aorta that appear as contrast-filled irregular outpouchings of the aortic wall.
- 40. Evaluation of pulmonary veins : In the context of electrophysiology interventions such as pulmonary vein isolation (PVI), preprocedural MDCT can be used to define pulmonary venous anatomy and identify supernumerary veins, and postprocedural MDCT can be used to evaluate for pulmonary vein stenosis. Additionally, in the setting of congenital heart disease, CT can be used to identify anomalous pulmonary venous return.
- 41. Evaluation of pulmonary embolism : MDCT is highly accurate in detecting PE, which appear as a filling defect in the pulmonary arteries. This modality is most sensitive for proximal (main segmental branches) thrombi, and small, distal emboli may be missed.
- 42. Valvular heart disease : Visualization of the valve leaflets, particularly the aortic valve, is feasible with newer- generation scanners due to their improved temporal resolution. Nonenhanced MDCT is also useful for assessing prosthetic mechanical valve leaflet motion.
- 43. Surgical planning : The utility of MDCT in surgical planning before cardiothoracic surgery, particularly for reoperations, is increasingly recognized. Preoperative scans can evaluate the proximity of mediastinal structures to the sternum (i.e., aorta, right ventricle, bypass grafts); the degree of aortic calcification (i.e., to guide cannulation sites); and concomitantly provide information about cardiac morphology (e.g., presence of a ventricular aneurysm). Ongoing studies are evaluating whether this added information might reduce intraoperative and perioperative complications.
- 44. Peripheral arteries : MDCT can also be used to evaluate peripheral arteries, including the carotid, renal, visceral, and lower-extremity vessels. Indeed, imaging these vessels is generally more straightforward than coronary imaging, due to their large caliber and minimal motion. CT can be used for planning and follow-up of vascular disease in these peripheral vascular beds.
- 45. Emerging Applications Detection of myocardial scar and viability Features suggestive of prior myocardial infarction and nonviable myocardium On first-pass imaging : ●Myocardial hypoattenuation (<50% of the surrounding myocardium) and, ●Myocardial thickness <5 mm. Late myocardial enhancement imaging with infusion of additional contrast medium and a delay of approximately 10 minutes. The kinetics of iodinated contrast material is similar to that of gadolinium, with accumulation within the interstitial space of myocardial fibrosis. Under delayed imaging, contrast preferentially accumulates within areas of scarring and can be detected on delayed imaging. Delayed enhancement on cardiac CT indicates regions of myocardium with reduced likelihood of functional recovery and patients whose ejection fraction will remain lower after myocardial infarction, particularly when a transmural pattern of delayed enhancement is present.
- 47. 2010 ACCF/AHA Guidelines for assessment of cardiovascular risk in asymptomatic adults Recommendations for Calcium Scoring Methods Class IIa Measurement of CAC is reasonable for cardiovascular risk assessment in asymptomatic adults at intermediate risk (10% to 20% 10-year risk) (Level of Evidence: B) Class IIb Measurement of CAC may be reasonable for cardiovascular risk assessment in persons at low to intermediate risk (6% to 10% 10-year risk) (Level of Evidence: B) Class III: No Benefit Persons at low risk (<6% 10-year risk) should not undergo CAC measurement for cardiovascular risk assessment (Level of Evidence: B) Recommendations for Coronary CT Angiography Class III: No Benefit Coronary computed tomography angiography is not recommended for cardiovascular risk assessment in asymptomatic adults (Level of Evidence: C)