Classification and causes of iron deficiency anemia
•Download as PPT, PDF•
0 likes•812 views

This document discusses classification and causes of anemia, focusing on iron deficiency anemia. It describes the normal iron metabolism process and requirements. Causes of iron deficiency anemia include blood loss, insufficient dietary iron intake, and malabsorption. Laboratory findings of iron deficiency anemia show a low hemoglobin with decreased MCV, MCH, and MCHC, known as a hypochromic microcytic blood film. The bone marrow appears hypercellular with increased red blood cell precursors that stain negative for iron.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Classification and causes of iron deficiency anemia
Similar to Classification and causes of iron deficiency anemia (20)
More from Ashok Moses
More from Ashok Moses (18)
Classification and causes of iron deficiency anemia
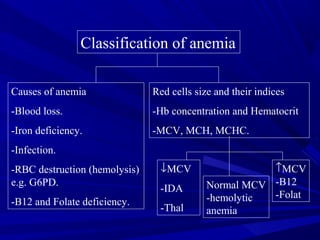
- 1. Classification of anemia Causes of anemia -Blood loss. -Iron deficiency. -Infection. -RBC destruction (hemolysis) e.g. G6PD. -B12 and Folate deficiency. Red cells size and their indices -Hb concentration and Hematocrit -MCV, MCH, MCHC. ↓MCV -IDA -Thal ↑MCV -B12 -Folat Normal MCV -hemolytic anemia
- 2. Iron deficiency anemia Normal iron metabolism: -The primary function is oxygen transport. -Iron is absorbed by duodenum and jejunim -Average total body iron content 3500-4000 mg. -Approximately 2/3 found in hemoglobin, -Iron is also stored in RE cells (BM, Spleen and liver) as hemosiderin and ferratin. -Also iron found in myglobin and myeloperoxidase and in certain electron transfer. -Iron is more stable in ferric state (Fe+++ ) than in ferrous state (Fe++ ).
- 4. Iron + Hem Iron Metabolism
- 5. Iron Absorption 1-2 mg only Plasma Fe Transferrin carriers 4 mg Body stores 1000 mg (M) 300-500 mg (F) Myglobin 300 mg 20 mg Fe Returned to immature RBC in BM RBC 2500 mg R.E. 20 mg Released daily Via RE system 90% extra vascular 5-10% intra vascular Loss (from GI tract) 1-2 mg daily Daily Fe++ turnover continuous process
- 6. Dietary iron: Iron is present in food as ferric hydroxides (ferric-protein complexes and hem-protein complexes). -meat, liver -vegetables, eggs. -The average diet contains 10-15mg and only 5-10% is normally absorbed. Iron requirements: It varies depending on sex and age: Male/female 0.5-1 mg/day Pregnant female 1-2 mg/day Children 0.5 mg/day
- 7. Clinical features: • When ID is developing, the RE stores (hemosiderin and ferritin) become completely depleted before anemia occurs. • At an early stage, no clinical abnormalities. • Later, patient may develops general symptoms and signs of anemia. • In severe case of IDA ridged or spoon nails.
- 8. Causes: • Chronic blood loss Fetomaternal Hemorrhage, inherited bleeding disorders menstrual peroid. • Maternal iron deficiency (neonate). • Growth spurts (infants and children). • Gastrointestinal, peptic ulcer, aspirin ingestion, carcinoma, hookworm, colitis, piles etc. • Pregnancy • Rarely hematouria, self-inflicted blood loss, hemoglobinuria. • Insufficient daily iron intake (poor diet). • Malabsorption.
- 9. Laboratory findings: •Red cell indices: Low Hb conc. MCV, MCH, MCHC* ↓ •Blood film: Hypochromic microcytic Picture. Occasional Target cells. Pencil shaped poikilocytes. Normal reticulocyte count. •Bone marrow iron: Normal to hypercellular. RBC precursors are increased in number. Iron stain negative. •Chemical testing on serum: Serum iron Decreased Transferrin/TIBC Normal to High Serum ferritin Decreased (Very low)
- 10. Hypochromic Microcytic picture (IDA) -ve BM Iron Stain +ve
- 12. Reticulocytes