
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Wilms tumor
Similar to Wilms tumor (20)
Recently uploaded
Recently uploaded (20)
Wilms tumor
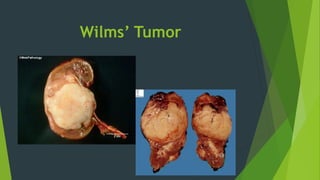
- 1. Wilms’ Tumor
- 2. Epidemiology Wilms tumor is the most common malignant renal tumor of childhood. Most diagnoses between 1 and 5 years with the peak incidence at age 3. Nearly 97% of Wilms’ tumors are sporadic, in that they occur in the absence of a heritable or congenital cause or risk factor. A hereditary form of Wilms tumor may be associated with bilateral presentation. Many congenital anomalies are associated with Wilms tumor, including WAGR syndrome (Wilms tumor, aniridia, genitourinary malformation, mental retardation),Beckwith-Wiedemann syndrome and some other overgrowth syndromes.
- 3. Clinical Manifestations Abdominal Mass(often painless) Abdominal Pain Hypertension Hematuria Obstipation Weight Loss Hypotension Fever
- 4. Laboratory & Imaging Studies CBC Liver & Renal Function Tests Ultrasound(should be performed to evaluate the presence of renal vein or vena caval extension.) CT
- 9. Differntial Diagnoses Hydronephrosis Polycystic disease of the kidney Mesoblastic nephroma Hamartoma Renal cell carcinoma Neuroblastoma Lymphoma Retroperitoneal rhabdomyosarcoma
- 10. Staging of Wilms’ tumor Stage I: Tumor limited to the kidney and completely excised. Stage II: Tumor that extends beyond the kidney but is completely excised. No residual tumor is apparent at or beyond the margins of excision. The tumor was biopsied, or there was local spillage of tumor confined to the flank. Stage III: Residual tumor confined to the abdomen. Lymph nodes in the renal hilus, the periaortic chains, or beyond contain tumor. Diffuse peritoneal contamination by the tumor, such as by spillage of tumor beyond the flank before or during surgery or by tumor growth that has penetrated through the peritoneal surface. Implants are found on the peritoneal surfaces. Tumor extends beyond the surgical margins either microscopically or grossly. Tumor is not completely resectable because of local infiltration into vital structures. Stage IV: Hematogenous metastases Stage V: Bilateral renal involvement
- 12. Treatment Before operation, all patients suspected of having Wilms’ tumor should undergo abdominal and chest CT. National Wilms’ Tumor Study Group (NWTSG) supports a strategy of surgery followed by chemotherapy in most instances, whereas the International Society of Paediatric Oncology (SIOP) approach is to shrink the tumor using preoperative chemotherapy. The goal of surgery is complete removal of the tumor Typically a transverse abdominal incision is made, and a transperitoneal approach is used.
- 13. Prognoses In general prognoses is very good. Prognostic factors include stage and histologic features. Cure rates for patients with localized Wilms tumor at diagnosis are greater than 85%, whereas patients with pulmonary metastases have event-free survival rates of approximately 70% to 80%.
- 14. References 1-Schwartz’s Principles of Surgery Tenth Edition 2-NELSON ESSENTIALS OF PEDIATRICS, SEVENTH EDITION 2015
- 15. Thanks