Femtosecond Laser Cataract Surgery Guide
•Download as PPTX, PDF•
54 likes•16,575 views

Femtosecond lasers emit extremely short pulses that can precisely cut tissue without damaging surrounding areas. They are used for cataract and refractive eye surgery. For cataracts, the laser creates incisions and fragments the lens for removal. For refractive surgery, it cuts corneal flaps and lenticules, improving precision over mechanical methods and reducing complications. While increasing costs and complexity, femtosecond lasers provide improved safety and accuracy for vision correction procedures.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Femtosecond Laser Cataract Surgery Guide
Similar to Femtosecond Laser Cataract Surgery Guide (20)
More from Anuraag Singh
Recently uploaded
Recently uploaded (20)
Femtosecond Laser Cataract Surgery Guide
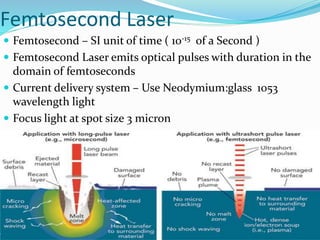
- 1. Femtosecond Laser Femtosecond – SI unit of time ( 10-15 of a Second ) Femtosecond Laser emits optical pulses with duration in the domain of femtoseconds Current delivery system – Use Neodymium:glass 1053 wavelength light Focus light at spot size 3 micron
- 2. Mechanism of Action Principle of photodisruption Laser energy is absorbed by tissues which result in plasma formation Expansion of plasma creates cavitation bubbles which separates the tissue plane
- 3. Micro vs Femto second laser
- 4. Femto second laser assisted cataract surgery Femtosecond laser first FDA approved for cataract surgery in 2010. With guidance systems it is used to make- Cataract clear corneal incisions Capsulorhexis Lens fragmentation/softening
- 5. Preoperative evaluation Special attention to • Corneal opacities • Arcus senilis • Pupil size • Zonular dehiscence • Grade and type of cataract • Patient should be told that operating procedure may take place in two different rooms
- 6. Anaesthesia Topical is preferred Encourage to look at fixation light Peribulbar blocks may cause chemosis and hinder docking GA in very young children
- 7. Instrumentation Alcon LenSx AMO Catalys Technolas Victus LensAR Three basic instrumentaion- 1. Patient interface 2. Laser delivery 3. Imaging system
- 8. Patient Interface 3 basic function Maintain positional and mechanical stability of eye Coupling device to facilitate laser delivery Permit acquisition of images Two types Applanating ( LenSx and Victus ) Small diameter Suitable in small palpebral aperture Nonapplanating ( Catalys and LensAR ) Cause less increase in IOP Less SCH
- 10. Imaging system Imaging system based upon- Spectral domain optical coherence tomography 3-dimensional confocal structural illumination
- 11. Imaging System Most important step is centering the cornea Corneal incisions and capsulorhexis
- 12. Capsulorhexis Ideally centered on limbus Can be centered on pupil ( set to 5mm )
- 13. Lens fragmentation 4-8 segments Concentric pattern in softer cataracts Grid pattern in harder cataracts Done before making the corneal incisions
- 14. Planning Station Incisions Position of primary and secondary incisions according to surgeon’s convenience Can be according to pre-op astigmatism Followed by Phacoemulsification
- 15. Contraindications Small palpebral aperture Interface diameter 11.5 to 15.5mm Can be overcome by lateral canthotomy Neck and back problem Optimal docking, imaging and laser delivery need patient to lie flat Nystagmus and attention deficit disorder Not able to comply instructions and fixation Glaucoma Rise in IOP 10-20 mmHg
- 16. Contraindications Corneal opacities Hinder in imaging Subluxated/Dislocated lens Nucleus management not possible Corneal incision can be made Liquefied lens material hinders laser penetration and incomplete capsulorhexis Small Pupils Relative contraindication Pupil expanding devices No air bubble should be in the AC
- 17. Unique Complications Machine related Errors in software or hardware Stop/reattempt Switch over to conventional Phaco Loss of suction Improper docking/excessive eye or head movement Hard head rest are preffered If occurs during capsulorhexis , complete manually SCH More in applanation type
- 18. Unique Complications Pupillary constriction Miosis of 2-3 mm Applanation/laser energy Incomplete capsulotomy/Anterior capsular tear Corneal folds/lens tilt/eye movements while firing laser Capsular block syndrome Intraoperative capsular block with subsequent rupture during hydrodissection Nucleus can be rotated by pneumodissection ( air bubbles produced by laser delivery )
- 19. Advantages Incisions Greater stability Capsulotomy More precise Better IOL centration
- 20. Advantages Nucleus management and phaco energy - Reduced ultrasound energy - Reduced effective phaco time Zonular weakness - Reduced stress on zonules during capsulorhexis and nucleus chopping Mild decentration capsulorhexis can be centered on lens Posterior capsulorhexis In infants Macular edema Lesser edema in comparison to phaco
- 21. Disadvantages Cost Training of staff – calibrate and operate the machine Operating room – shifting of patient may be inconvenience Time – two step procedure, takes longer time then phaco Increased expectation- more expensive more expectations
- 22. Femto Second Laser Refractive Surgery Femtosecond laser first FDA approved for LASIK flaps in 2001 1st released commercial device was: Intralase FS™ (Abbott Medical Optics, Abbott Park, Illinois); Femtec® (20/10 Perfect Vision, Heidelberg, Germany); VisuMax Femtosecond System® (Carl Zeiss Meditec, Jena, Germany); Femto LDV™ (Ziemer Group, Port, Switzerland); and Wavelight FS200®
- 24. Intralase Femto lasik Technique: The suction ring is centered over the pupil. The docking procedure is then initiated while keeping the suction ring parallel to the eye.
- 27. Flap raised with blunt spatula Suction is then released. A spatula is carefully passed across the flap starting at the hinge and sweeping inferiorly to lift the flap for excimer laser ablation.
- 28. Advantages: Reduced incidence of flap complications like buttonholes, free caps, irregular cuts , wrinkles as seen in LASIK. Diffuse lamellar keratitis
- 29. Advantages Decreased incidence of Subepithelial Haze Epithelial ingrowths
- 30. Advantages Control over flap diameter and thickness, side cut angle, hinge position and length. Increased precision with improved flap safety and better thickness predictability. Capability of cutting thinner flaps to accommodate thin corneas and high refractive errors. Stronger flap adherence. Less increase in IOP required Lesser incidence of dry eye. Lesser hemorrhage from limbal vessels. The ability to retreat immediately if there is incomplete FS laser ablation.
- 31. Disadvantages: Opaque bubble layer (OBL): Gas bubbles routinely accumulate in the flap interface during FSL treatment May dissect into the deep stromal bed(obscuring excimer laser tracker) Reach AC, or escape to subepithelial (resulting in button hole).
- 32. Patients present with extreme photophobia and good visual acuity Proposed mechanism is either an inflammatory response of the surrounding tissue to the gas bubbles or biochemical response of the keratocytes to the near-infrared laser energy Resolves without sequel but requires aggressive topical steroids for weeks. Micro-irregularities on the back surface of the FSL LASIK flap can cause “rainbow glare”
- 33. Rainbow glare
- 34. Disadvantages Photodisruption-induced microscopic tissue injury and ocular surface inflammatory mediators may cause lamellar keratitis in the flap interface. Increased difficulty in lifting the flap if retreatment is required after that (because of good adherence). Increased cost. Moving the patient between 2 laser instruments.
- 35. Intrastromal lenticule extraction ReLEx (refractive lenticule extraction) Performed exclusively with a femtosecond laser system, i.e., no excimer laser is needed. Steps:. The femtosecond laser is used to cut a small lens-shaped segment of tissue (lenticule)within the center of the cornea.. Made in the anterior cornea with the laser — similar to the flap created in LASIK. The flap is lifted and the lenticule is removed and discarded.. The flap is repositioned The removal of the lenticule reduces the curvature of the cornea, thereby reducing myopia.
- 37. SMILE A variation of ReLEx is another investigational procedure called small-incision lenticule extraction (SMILE). In the SMILE procedure, a corneal flap is not created. A small incision is made in the mid-periphery of the cornea with the laser, and the lenticule is removed through this self-sealing incision. The SMILE procedure has additional potential advantages. No corneal flap is created, SMILE may pose less risk for post-surgical dry eye and ectasia than ReLEx or LASIK. No risk of flap displacement from trauma to the eye after surgery.
- 38. SMILE The promising early results of ReLEx and SMILE suggest they may someday become a popular alternative to LASIK for vision correction. However, currently it is not possible to perform these procedures for small amounts of ametropia, as typically present in enhancement surgery, because the lenticule would be too thin to manipulate safely.
- 39. Intracor